CHAPTER 25 SAFELipo for Men
Summary
SAFELipo was introduced by the senior author in 2002 to address the limitations of traditional liposuction. SAFELipo is an acronym describing this comprehensive process approach to fat management: Separation, Aspiration, and Fat Equalization. The separation phase mechanically emulsifies and liquefies the targeted adipose tissue prior to any suction. By liquefying the targeted adipose tissue, this fat is differentiated from the surrounding “solid” fat and supporting vessels and stromal network. The targeted fat is aspirated preferentially, leaving the superficial fat and supporting structures intact, unlike typical liposuction that avulses blood vessels and supporting structures along with the relatively solid fat. The process approach of separation of fat followed by preferential aspiration allows greater control, precision, and safety. Recognizing that perfectly even adipose removal can never be achieved, fat equalization, the final step of SAFELipo, emulsifies some of the remaining fat that will serve as local fat grafts to fill in any imperfections. By comparison, traditional liposuction works by punching holes throughout the adipose latticework to weaken and collapse the fat, and then hoping that the skin collapses evenly. With SAFELipo, even if some irregularities exist after aspiration, the equalization phase will correct and prevent deformities. When properly understood and utilized, SAFELipo can go beyond aspiration lipectomy. Expansion vibration lipofilling (EVL) was developed in conjunction with and as a complement to SAFELipo to provide a more effective and potentially safer way to transfer autologous fat. SAFELipo and EVL can correct iatrogenic contour deformities and dramatically alter silhouettes through addition, subtraction, and redistribution while controlling skin redraping. This chapter covers both the techniques for SAFELipo and EVL.
Introduction
The goal of liposuction is to precisely and evenly extract the “desirable” solid fat matter that is contained within a sandwich of “undesirable” structures, exploiting the differential resistance of these tissues. This concept has been the foundation of successful liposuction since it was originally introduced by Illouz in 1977. 1 Low-resistance adipose tissue is more easily disrupted and aspirated relative to the higher-resistance vessels, stromal-supporting network, overlying skin, and underlying musculocutaneous structures. Tactile feedback allows the surgeon to detect cannula misguidance and keep the cannula in the safe, low-resistance adipose tissue. While this simplified explanation of why liposuction works allows for the avoidance of vital structures and aspiration of fat, it does not address the uneven and nonuniform removal of fat as we have known it for decades. Despite many advances in the field of blunt cannula extraction of fat (liposuction), especially in the area of patient safety, the basic problem with liposuction was not overcome—the dose–response curve of liposuction. The more fat that is removed from an area (the dose), the higher the tendency toward creating a contour deformity (the response). Surgeons have subsequently become experts at incompletely removing fat to avoid creating contour deformities, or in other words, learning to take just enough fat to make patients happy while not creating obvious contour deformities. Many devices and technologies have been proposed over the years that would supposedly allow for blunting, or even the elimination of this dose–response curve, none of which appear to have been effective. In fact, the opposite is true, where the development of thermal means of liposuction has contributed additional means of creating scar tissue and resultant contour deformities because of the thermal load imparted to the delicate supporting stromal tissues. The penetration or disruption of these supporting structures has been the source of many complications through the decades, the most frequent of which is the development of contour deformities after liposuction. These disruptions have been the source of many complications through the decades, the most frequent of which is the development of contour deformities after liposuction. To improve the safety and efficacy of liposuction, the resistance differential needs to be widened and exploited maximally to allow greater precision of aspiration. When the differential is narrow, vessels and unwanted superficial fat are avulsed. The goal is a controlled, smooth laminar removal of a sheet of subcutaneous fat so that the overlying superficial fat and dermis redrape naturally over the deeper musculoskeletal structures, without dermal adherence to the underlying tissues. However, because the procedure is blind, we can approach but never achieve perfectly even adipose removal. Acceptance of the imperfect removal is critical to preventing iatrogenic contour deformities.
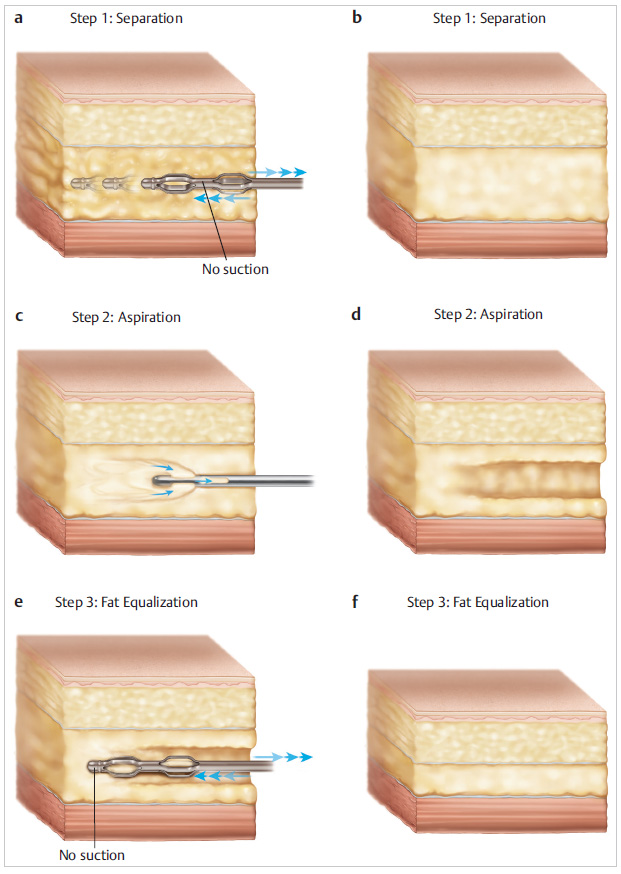
SAFELipo was introduced by the senior author in 2002 to address the limitations of traditional liposuction. 2 , 3 SAFELipo is an acronym describing this comprehensive process approach to fat management: Separation, Aspiration, and Fat Equalization. 2 The foundation of SAFELipo is widening the resistance differential, which gives the surgeon greater control and precision in manipulating the adipose tissue. The separation phase mechanically emulsifies and liquefies the targeted adipose tissue prior to any suction ( Fig. 25.1 ). By liquefying the targeted adipose tissue, this fat is differentiated from the surrounding “solid” fat and supporting vessels and stromal network. The targeted fat is aspirated preferentially, leaving the superficial fat and supporting structures intact, unlike typical liposuction that avulses blood vessels and supporting structures along with the relatively solid fat. The process approach of separation of fat followed by preferential aspiration allows greater control, precision, and safety. Recognizing that even adipose removal can never be achieved perfectly, fat equalization, the final step of SAFELipo, emulsifies some of the remaining fat that will remain and serve as local fat grafts to fill in any imperfections. The equalization phase becomes more critical in thinner patients when small discrepancies in tissue thickness become more readily visible externally. By comparison, traditional liposuction works by punching holes throughout the adipose latticework to weaken and collapse the fat, and then hoping that the skin collapses evenly. With SAFELipo, even if some irregularities exist after aspiration, the equalization phase will correct and prevent deformities. Separation and equalization also soften and relax the deep septal stromal network that runs throughout the subcutaneous layer and allows for recruitment or decruitment of the overlying skin, seen externally as smooth skin without dermal or fascial adherences. These rigid subcutaneous adherences tether the skin and are another etiology of contour irregularities. By relaxing the attachments of the skin to underlying structures, the skin can be predictably manipulated and redistributed as needed from areas of excess into areas of deficiency and vice versa. When properly understood and utilized, SAFELipo can go beyond aspiration lipectomy. The principles of SAFELipo have been extended to comprehensively manage volume and control skin redraping. EVL was developed in conjunction with and as a complement to SAFELipo to provide a more effective and potentially safer way to transfer autologous fat. 4 SAFELipo/EVL can correct iatrogenic contour deformities and dramatically alter silhouettes through addition, subtraction, and redistribution while controlling skin redraping. 4
It is worth discussing that thermal methods of liposuction (laser, ultrasonic, radiofrequency, and others) dramatically reduce cannula resistance within the tissues indiscriminately, narrowing the resistance differential between targeted and unwanted tissues. Thereby, surgeon precision is compromised, as the tactile feedback is blunted. Additionally, these devices create a significant scar burden, and as the skin redrapes postoperatively, the fibrosis generated predisposes the patient to unnatural contours and dermal adherences that result in visible contour deformities.
Physical Evaluation
Hernias: Failure to recognize facial defects can lead to inadvertent intra-abdominal cannula passage and bowel injury.
Skin quality: Successful liposuction depends on skin retraction to the reduced framework. Assess skin elasticity and striae. Non-Caucasian patients tend to have better skin contraction postoperatively.
Fat distribution pattern: Differentiate and point out intra-abdominal from extra- abdominal fat. Also, note the patient’s adipose distribution pattern (apple vs. pear, etc.) and distribution asymmetries.
Muscular framework: Evaluate muscle bulk and definition and patient goals of muscular definition (lean/thin vs. big/broad).
keletal asymmetries: Scoliosis, leg length discrepancies, pelvic tilt, and chest wall deformities should be documented and discussed with the patient.
Body mass index (BMI): Patients with a BMI over 30 typically have a large amount of intra- abdominal fat, and it is more challenging to create a pleasing result and a satisfied patient. We encourage patients to get healthier and try to postpone surgery until their BMI is under 30.
Suprapubic fat: To create a harmonious anterior torso, lipodystrophy of the mons area cannot be ignored. In males, reduction of mons adiposity will increase penile shaft exposure, which can be an added benefit for many patients.
Cellulite: Cellulite represents a mechanical imbalance of superficial fat volume relative to the compliance and elasticity of the investing fibrous septal chambers.
Zones of adherence: If treating adipose adjacent to these zones, these adherences need to be softened and broken up to create a smooth contour.
Anatomy
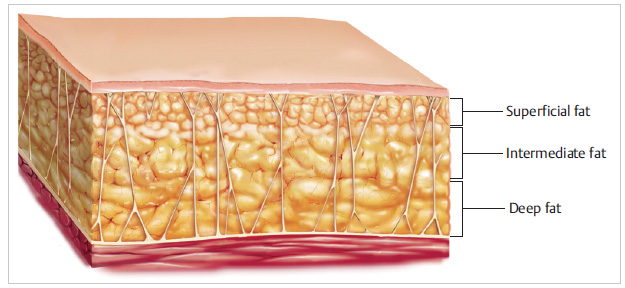
The anatomy of subcutaneous fat is traditionally divided into a superficial and deep compartment, separated by Scarpa’s fascia or the superficial fascial equivalent. The superficial adipose layer has dense, compact fat within tightly organized fibrous septa, while the deeper fatty layer is more loosely arranged and more areolar.5 Clinically, because liposuction is blind, it is more useful to manage the fat from the perspective of depth relative to the skin rather than with respect to Scarpa’s fascia. Although somewhat arbitrary and simplified, we divide the subcutaneous fat into three layers: superficial, intermediate, and deep 6 ( Fig. 25.2 ).
The deep and intermediate layers are safer and easier to treat, while the superficial adipose layer requires more precision. Irregularities in the deep layer can sometimes be disguised by superficial fat, but inconsistencies in the superficial layer of fat will predictably create deformities. Because the superficial fatty layer is more fibrous and closer to the skin surface, laminar extraction is more difficult and irregularities are less forgiving. This is not to say that the superficial compartment must be avoided and cannot be safely manipulated. We treat the superficial compartment routinely to create more anatomical definition (semilunar line, male chest wall sculpting, etc.). With SAFELipo, more fibrous areas can be safely accessed if the surgeon increases the separation and equalization phases.
Zones of adherence represent areas with thicker and stronger fibrous connections between the skin and the underlying deep fascia. Some authors recommend avoidance of liposuction of these areas, because they are predisposed to postoperative irregularities. 7 However, if identified preoperatively, the stiff fibrous connections can be relaxed with separation and equalization. The tissue will become more pliable allowing the skin to redrape naturally, and the whole area can be treated safely and successfully.
Cellulite has two etiologies—both are the result of a mechanical disharmony. In the superficial fat compartment, fat is tightly packed within fibrous compartments. Septa run from the skin to the superficial fascia with limited ability to expand and contract. The primary type of cellulite, as described by Illouz, 8 is caused by compartmental fatty hypertrophy with the septa tethering the skin to the fascia, creating compartment bulges. Treatment of this type of cellulite is aimed at either reducing the fat within the compartment or obliteration of the septal anchor points. Lockwood describes the second type of cellulite as a result of skin and fascial laxity: “With age and sun damage, the entire skin–superficial, fat–superficial fascial system (relaxes and stretches, resulting in ptotic soft tissues, pseudo-fat deposit deformity, and cellulite.” 9 This second type of cellulite is most common with massive weight loss patients and older age and is surgically corrected by tightening the skin and fascial system.
Steps for SAFELipo for Men
Trunk liposuction using the SAFELipo process is typically performed in three positions: supine, and both the left and right lateral decubitus positions. Although evidence is currently lacking, turning the patient multiple times, including into the lateral decubitus position, may reduce the risk of deep vein thrombosis and pulmonary embolism, because venous pressure is decreased on the elevated side, decreasing pooling and improving pelvic venous drainage. Adequate padding of all pressure points is important, along with careful sterile prepping and draping. A single whole-body prep is preferable, with the sterile field extending from the neck down to the end of the bed, so that the patient can be moved into different positions during the procedure without the need for further prepping.
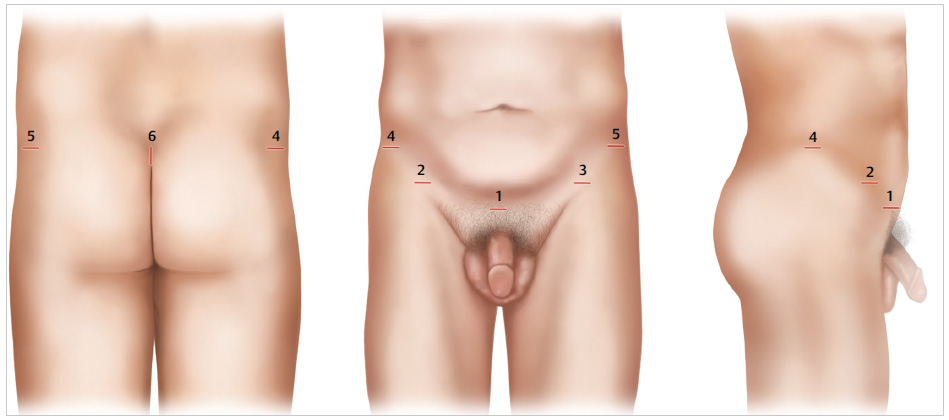
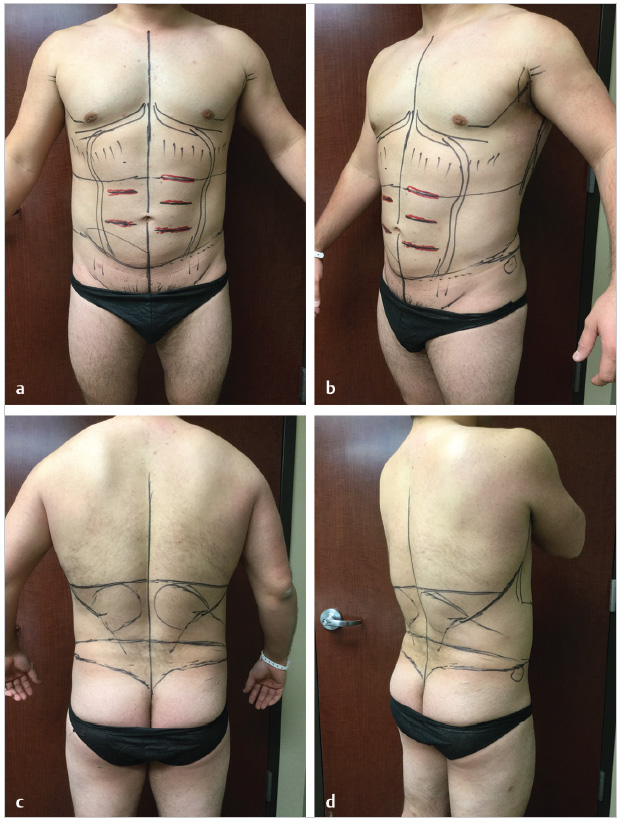
Performing liposuction from these three positions, supine, and right and left lateral decubitus, can help prevent contour deformities, including “shark bites” in the midbuttocks and other stigmata of liposuction that are seen frequently. Some surgeons perform the procedure with the patient in a somewhat supine position, but with the legs pulled up and across the body, which will create an unnatural appearance of the trunk, hips, buttock, and lateral thigh because of the twisting of the spine and the bulging prominence of the femoral trochanteric area. Performing contouring in this nonanatomical position of the buttock and lower extremities can lead to overcorrection or undercorrection, which are frequently seen as contour deformities of the midbuttock, gluteal crease, and lateral thigh areas. In the lateral decubitus position, the normal, standing position is most closely resembled, allowing contouring to match the same position in which the patient evaluates herself or himself at home in front of a mirror. Additionally, the lateral decubitus position allows thorough treatment of the upper abdominal area, whereas the supine position often does not as a result of the abdomen being hyperextended in the supine position, creating interference from the underlying rib cage and adherence of the tightened abdominal skin to the underlying framework. In the lateral position, the patient’s upper abdominal skin can be freely pulled away from the underlying ribs, which are now less protuberant because of the more flexed abdominal position. There is also an element of added safety in performing the upper abdominal work with the patient in the lateral decubitus position, because the ribs are not constantly presenting themselves with the potential to penetrate beneath them. Treating the target areas from multiple positions and multiple access sites increases cross-hatching and reduces irregularities ( Fig. 25.3 ).
In any liposuction procedure, adequate infusion of the wetting solution is crucial to minimizing blood loss, providing additional anesthesia, and increasing working space through volume expansion. In primary cases, a typical superwet infusion is used, with an infusion-to-aspiration ratio of 1:1 or 1.5:1.
In a repeat liposuction procedure, in which volume expansion of the target zone is even more vital to being able to adequately traverse the tissue planes, a tumescent approach with a ratio of 2:1 or even 3:1 is frequently needed. In the past, a Klein needle was used for this important aspect of the procedure, encompassing an infusion phase and then roughly 20 minutes of waiting to allow maximum vasoconstriction of the tissues before performing step 1 of the SAFELipo process, separation.
In collaboration with the senior author (S.W.) and in the course of applying SAFELipo concepts to his liposuction and fat-grafting procedures, Dr. Daniel Del Vecchio first proposed the utility of performing SST. 4 The time needed for maximum vasoconstriction to take effect is drastically reduced by simultaneously infiltrating the wetting solution while performing step 1, separation. With a classic Klein needle and slow manual movement of the needle, the wetting solution will disperse into the areas of least resistance, and large depots of wetting solution are created typically at the fat–fascia interface, deep to the targeted subcutaneous tissues and their associated capillary networks. However, for maximal efficacy of the epinephrine, the solution should be evenly dispersed throughout the entire subcutaneous space to maximize the surface area and contact between the solution and targeted small blood vessels. SST separates the tissues and creates a latticework of low-resistance tissue planes for wetting solution dispersion and vasoconstriction. For SST, we use an angled, exploded-tip 3-mm cage cannula, which is connected to the power-assisted device and the tumescent solution pump.
After SST, additional separation of targeted fat is usually desired. Step one, separation (including SST), accounts for approximately 40% of the total procedural time. Fat separation is typically performed using PAL to maximize the oscillations and efficacy of the wings on the exploded-tip cannulas and to minimize effort during liposuction ( Fig. 25.4 ). Although PAL makes SAFELipo less strenuous, more accurate, and much more efficient, SAFELipo can be accomplished manually without power. The angled cannulas or dissectors have a blunt tip and “wings” or baffles that create relatively high- and low-pressure zones when passed through tissue. These moving zones of tissue pressure gradients adjacent to the cannula wings allow fixed fat globules to dislodge and detach from their surrounding attachments, essentially separating these droplets of fat from each other and from their supporting networks of blood vessels and stromal tissues. This process of mechanical emulsification, or separation, changes the normally solid fat architecture into a more liquid environment in the targeted areas, in effect creating a treatment zone of low-resistance emulsified fat, leaving higher-resistance untreated areas above (skin) and below (musculoskeletal structures). The creation of this differential in these treatment planes is crucial to being able to safely and easily navigate through the area during step 2, spiration.
In a repeat liposuction case, the widening of differential tissue resistance is even more important, because the natural differential in resistance between the fat layer and its overlying skin or underlying musculoskeletal structures has disappeared as a result of scar tissue from previous liposuction. Advocates of thermal liposuction (laser, ultrasound, radiofrequency) argue that these repeat cases are ideal for energy-based liposuction technologies. However, in our experience, these are the worst cases for thermal liposuction. Thermal liposuction devices indiscriminately lower cannula resistance and blunt the surgeon’s tactile feedback to stay in the correct tissue plane. In a typical repeat liposuction case, there is already a fibrotic bed and a more solid architecture of scar tissue, fat, and supporting structures; this typically manifests to the surgeon as an inability to pass an infiltration or liposuction cannula through the tissues. Longer treatment time and a higher thermal load are imparted to the tissue bed, increasing inflammation and subsequent scarring and, in some cases, causing outright burns. Even with the use of traditional liposuction in repeat cases, end-hits to the skin or damage to deeper structures are much more common and can give unfavorable results.
Using SAFELipo, the separation step allows the surgeon to regain the lost differential in resistance between these planes, allowing for easy navigability through the target zones, whether the goal is to remove more fat, redistribute what remains, or add more fat to the area using EVL. For example, if additional fat is to be removed, it is easy to remain within the targeted zone of separated, excess fat, because its resistance has been made noticeably lower than the overlying skin and underlying bed, similar to the feel of a typical primary liposuction procedure. The supporting structures and blood vessels are spared, because they remain solid and distinct from the targeted, emulsified fat that is preferentially aspirated.
There is no need for any thermal energy or suctioning during step 1, separation, so tissue and blood vessels surrounding the fat are left intact. Separating the fat has been compared with shaking an apple off the tree, a relatively gentle procedure. It is important to define the proper plane to prevent misadventures and avulsion injury to vessels or destruction of the stromal network. As previously mentioned, PAL facilitates a more expedient procedure, maximizing the amount of fat separation that can be accomplished with each pass. The desired end point at this stage is loss of resistance of all targeted fat, showing the operator that the target zone is adequately mechanically emulsified.
Only after separation of the targeted fat from its attachments is achieved, a more conventional cannula (e.g., a 2.7-, 3-, or 4-mm angled long-port double Mercedes wall cannula) with smaller, less aggressive, and more numerous ports is used to aspirate the now “emulsified” low-resistance fat. Because the fat has already been separated, this aspiration process is fast and almost entirely bloodless and can be accomplished with smaller, less aggressive cannulas that cause minimal trauma to the surrounding fat, vasculature, and stromal network left behind, which is necessary to provide a smooth, natural contour that will heal uneventfully. Step 2, aspiration, usually constitutes approximately 40% of the total treatment time.
Similar to how water is sucked with a straw out of a glass of water with ice cubes, this mechanically emulsified or liquefied fat is suctioned preferentially out of the subcutaneous layer, leaving behind an intact supporting network. In contrast, standard liposuction uses tremendous negative pressure to forcibly avulse fat and supporting structures in their natural, solid, high-resistance state. Because the targeted solid fat and the supporting blood vessels have similar tissue resistance, they are both aspirated at nearly equivalent rates.
The third step of SAFELipo is fat equalization. Similar to step 1, fat equalization is performed without any suction and with the same exploded-tip cannula or dissector. Step 3 typically constitutes approximately 20% of the total procedural time. When first using the SAFELipo process, many practitioners find that they spend less time in step 1 but far more time in step 3, trying to equalize the remaining bed. As experience is gained and the importance of step 1 is fully realized, the 40/40/20 time split is more common. In repeat liposuction procedures, more time is typically spent trying to equalize remaining hills and valleys, through aggressive molding and contour equalization of the remaining fat bed with the opposite hand in conjunction with moving the exploded-tip instrument back and forth through the uneven tissue bed. Additionally, EVL is almost universally utilized to equalize the volumes of these challenging cases.
The fat equalization step effectively separates some of the remaining fat, eliminates thicker and thinner areas of fat, and leaves this newly separated fat as a smooth layer of “local” fat grafts that prevent adherence of the dermis down to the deeper fascia or other musculoskeletal structures. This blanket of “local” fat grafts is left in place to buffer against scarring, skin adhesions, and their resultant contour deformities. This smooth and even layer of local fat grafts provides the smoothness and natural appearance typically seen in SAFELipo procedures even when the remaining layer of fat is left very thin, which is in sharp contrast to other forms of liposuction that typically create unsightly contour deformities as the fat layer is made progressively thinner.
Fat equalization combines aspects of fat separation with fat shifting and “local” fat grafting to produce a smooth, even, and compliant remaining layer of fat for an aesthetically pleasing result. In the past, one of the biggest challenges of liposuction was how to remove all of the unwanted fat in an area without creating a dented, lumpy, or wavy surface in the treated area. The comprehensive process involved in SAFELipo has answered that challenge and seeks to create dramatic yet smooth and natural results.
For primary and repeat cases, the end point of the fat equalization step is a smooth rolling pinch test. Using both hands, and without using any instrumentation, the skin is gently pinched and rolled between the fingers and thumbs, rolling across the entire area in multiple different directions to assess the smoothness of the skin and underlying fat layer. In areas of persistent unevenness, the exploded-tip dissector can be inserted and pushed back and forth through the uneven area while pinching up the area with the opposite hand, applying gentle pressure to the uneven area. In repeat cases where the area is still not smooth, fat shifting and aggressive manual molding is performed, if needed, along with formal fat grafting (EVL) if the area is still volume deficient. Finally, the release of any remaining skin adhesions is performed in a conservative and precise fashion.
Most plastic surgeons are very familiar with the traditional spot approaches that have been widely taught and adopted to treat contour deformities. The technique proposes to treat hills with liposuction and valleys with fat grafting, and to leave alone areas that are neither hills nor valleys. These spot approaches typically require extensive preoperative markings and long procedure times through multiple access incisions. In stark contrast, equalizing an entire area with the SAFELipo process is technically much simpler to perform, with the added benefit of making formal fat grafting unnecessary in many cases. Rather than aspirate down the hills and fill in the craters, SAFELipo rakes across the entire area to allow the hill excess to be swept across and fill in the craters. If formal fat grafting is still needed, the SAFELipo process provides a receptive environment for the fat grafts, unlike the inhospitable and frequently hostile recipient bed seen after thermal methods of liposuction.
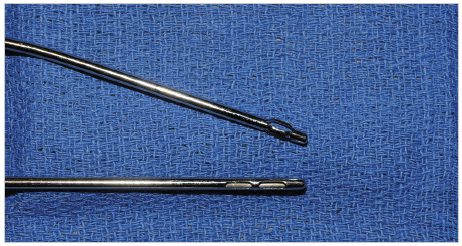
Several additional techniques are useful in helping to prevent contour deformities during liposuction. First, suction should be cut off before inserting and removing cannulas to prevent the creation of a depression at a cannula entry site. Also, angled cannulas are used exclusively, because they can be rotated and redirected without needing to retract the cannula back to near the entry point ( Fig. 25.5 ). This prevents digging holes and also allows more complete coverage of an area, with constant rotating of the angled cannula creating a “windshield wiper” effect and maximal coverage. Areas closest to the incision should always be treated last, and the fat should be carefully equalized at the access sites at the conclusion of the case. All access sites except the sites used for formal fat grafting are left open to drain, minimizing fluid accumulation, bruising, and persistent swelling. Finally, it is generally prudent to not suction the midbuttock area and gluteal fold area, and to frequently perform fat grafting on them to prevent further depression or collapse. The use of EVL allows for much more expansion and support of these areas than other fat grafting techniques.
Abdominal wall etching, first described by Mentz, 10 is an adjunctive contouring technique and is gaining interest among plastic surgeons and patients. Abdominal etching is the intentional creation of differential fat thickness in adjacent zones using liposuction. These areas can also be thought of as intentional iatrogenic contour deformities to give dimensionality and greater muscular definition. In muscular or athletic patients with little subcutaneous fat and visible abdominal wall musculature, it can accentuate the desired appearance of abdominal wall inscriptions, the linea semilunaris, and the linea alba ( Fig. 25.6 ). Problems arise when surgeons apply etching techniques to patients who do not have visible abdominal musculature at rest or flexing or in patients with excess skin. It is in these patients, or in patients who have gained a significant amount of weight after etching surgery, that we have seen the most problems. While abdominal etching results can look pleasing in a static fit patient, significant aesthetic problems can arise if a heavier patient’s body habitus does not align with etched abdominal musculature, or in patients who gain weight, or when some patients are observed dynamically. In some cases, the iatrogenic etches do not contract and move like the anatomy they are mimicking, and the heavier the patient, the greater this discordance.
In patients with less subcutaneous fat and clearly visible underlying abdominal musculature, we will perform extra equalization at the linea semilunaris and the linea alba to give the abdomen a better three-dimensional shape, but we perform this technique cautiously and only in this subset of patients. We recommend against this technique in obese patients with a thicker subcutaneous fat compartment and no visible abdominal muscular anatomy. In general, the superficial compartment should not be treated with etching if the deeper compartments have significant residual lipodystrophy. Abdominal etching is particularly difficult to control postoperatively, given that the abdomen is one huge flexion crease. Postoperative contour control with foam, proper compression, avoidance of flexion, and avoidance of unfavorable compression from tight clothing are all crucial in achieving favorable results in abdominal etching.
In contrast to the limited amount of patients who are candidates for abdominal etching, practically every male chest requires differential SAFELipo with or without pectoral enhancement with EVL for a natural and masculine shape. If the thoracic area is simply liposuctioned uniformly thin in all areas, it gives an unnatural and undesirable appearance with the chest appearing flat and amorphous without any contour. Just as the aesthetic female form requires breast shape, the aesthetic male form requires muscular shape to the chest. Similar to breast size preference in females, some men want more pectoral volume than others. To provide pectoralis muscle definition and shape anteriorly and latissimus muscle tone in the axilla, differential SAFELipo is used to leave some areas thicker than others ( Fig. 25.7 ). An L-shape is designed in the inferior lateral aspect of the chest and this L will be taken down very thin. The superior medial aspect of the chest will be left thicker to give pectoralis shape as needed. We often utilize EVL in the area of the pectoralis major for patients who need additional volume and shape. In the axilla, we aggressively excavate and thin out patients until we meet the anterior border of the latissimus; leaving some extra thickness over the latissimus can give males a more desired V-shape. After we finish SAFELipo of the entire chest and axilla, many patients still have residual glandular elements beneath the areola that need to be pulled out from the small access incision at the areola. When SAFELipo has been done correctly, this fibrous glandular tissue is no longer adherent to the surrounding tissues and can be pulled out very easily with a hemostat, either en bloc or in pieces ( Fig. 25.8 ).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


