CHAPTER 22 Boomerang Excision Pattern Correction of Gynecomastia
Summary
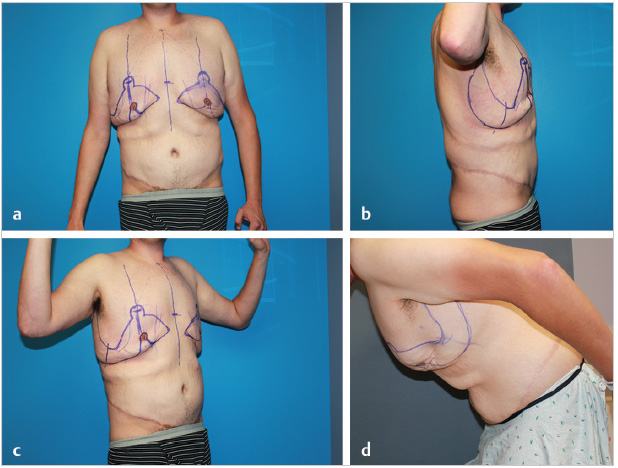
Boomerang excision pattern correction of gynecomastia is designed to simultaneously correct both gynecomastia and loose skin of the chest and upper abdomen. A J torsoplasty is usually added to complete the circumferential upper body lift. Boomerang pattern refers to the right angle elliptical skin excisions that straddle each nipple–areolar complex (NAC), thereby removing excess skin in both the vertical and horizontal planes while raising the ptotic nipples to their proper position. Several case presentations demonstrate the versatility of the boomerang pattern.
Introduction
After massive weight loss (MWL), men seek body contouring surgery for the removal of excess skin and fat followed by tightening and suspension of residual lax tissues through taut closure of excision sites. Most men have at least correction of pseudogynecomastia and an abdominoplasty with posterior extensions. 1 Muscular men desire correction of gynecomastia followed by upper body dominance and muscular show. This chapter presents original operations for moderately ptotic gynecomastia and upper torso skin laxity after MWL. 2 Chapter 40 addresses male total body lift, which is a collection of operations that include a boomerang pattern excision correction.
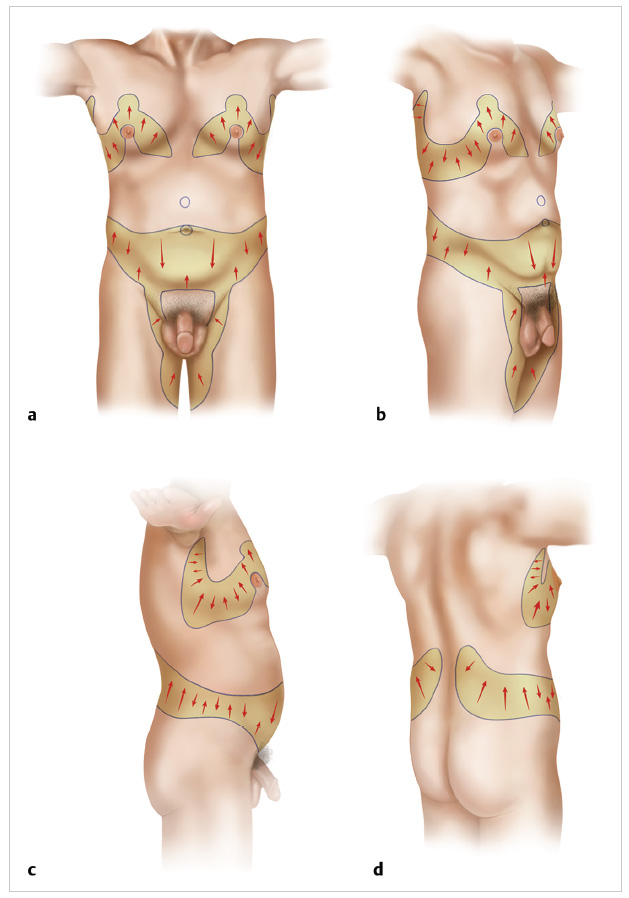
For the correction of gynecomastia and upper torso laxity, a boomerang pattern surrounds each nipple. The pattern consists of two large, asymmetric obliquely oriented elliptical excisions that drape superiorly over the nipple-areolar complex (NAC) at right angles. The wrap around the NACs resembles the Australian Aborigines’ aerial weapon and hence the name. Coupled with J torsoplasty extensions, these ellipses are designed large enough to correct the gynecomastia, nipple ptosis, inframammary fold (IMF) adherences, and circumferential upper torso skin laxity. Success in these combinations of operations fulfills the concept that both horizontal and vertical skin excess can be removed through a series of complimentary angled long oblique excisions 2 ( Fig. 22.1 ). The undulating scars do not cross the midline and appear interrupted as they encircle the superior NAC. The continuation through a lateral torsoplasty hides that portion of the body lift scar under the resting arm.
Popular midchest transverse excisions mostly remove vertical excess. 3 The long transverse excision and scar positioned along the prior IMF appears to simulate a new feminine IMF. The residual transverse skin redundancy of skin disappointedly hangs when leaning over. An inferior buried pedicle flap to nourish the NAC leaves too much inferior fullness. 3 When the pectoralis muscle contracts, inferior pole should be empty, but that cannot happen when there is an inferior buried pedicle.
Physical Evaluation
Size and composition of the palpable gynecomastia.
The extent of nipple ptosis as related to inferior lateral junction of the pectoralis muscle.
Magnitude of loose chest skin and excess adipose.
Delineation of the IMF.
Anatomy
Pseudogynecomastia after MWL is a pair of flaccid masses of soft tissue centered under vestigial nipples lying within a loose sheet of chest skin on a broad musculoskeletal framework. There are distinctly palpable transversely oriented sausage-like mobile masses with cores of pale and firm glandular tissue with tentacle-like extensions through adipose. The NAC positions lie some distance inferior to the lower border of the pectoralis major muscle. Their descent is restricted by IMFs formed by concentration of fibrous tissue extending along the fifth rib to some transverse line along the inferior breast dermis through relatively thin subcutaneous tissue. The expected fibrous adherences of the lateral and inferior pectoral border are obscured by adipose and/or skin sag. The male rib cage is barrel-like instead of a feminine upside-down cone. The organomegaly of the prior obesity accentuates upper body breadth. The humeral heads are further apart than the pelvic rims.
An important goal is to raise the inferior border of the new NAC slightly lateral to the midclavicular line to lay several centimeters superior to the inferior lateral pectoralis muscle junction.
Patient Selection
The indication for the boomerang pattern and J torsoplasty is moderate-to-severe gynecomastia with disturbing skin laxity of the upper torso. Mild deformity is treated with less scars by ultrasound-assisted liposuction of anterior chest with glandular pull-through resection along a periareolar incision. 4 Severe mid-torso skin excess is better treated with transverse excision and nipple skin graft. 1 , 4 At extreme nipple ptosis, the boomerang pattern will not work because there is too much skin inferior to the nipple, which will not stretch out when the nipple is transposed to its proper superior position. In all others, the boomerang pattern J torsoplasty works well, but the patient must accept long undulating chest scars. The ideal patient is muscular young males with considerable loose upper torso skin and sagging gynecomastia. Also suitable are less sinewy men who desire no residual excess skin in exchange for undulating oblique scars interrupted by the NAC. If the residual skin is anticipated to carry too much adipose, then the surgery should be delayed for further generalized weight loss.
Steps for Boomerang Pattern Correction for Gynecomastia
The boomerang excision pattern consists a symmetrical pair of two asymmetrical elliptical excisions that drape at right angles superiorly over the NACs ( Fig. 22.2 ). They are created large enough to correct both the gynecomastia and treat mid-torso skin laxity. For this complex pattern to be applied, the plastic surgeon designs the excisions by pushing and grasping the tissues ( Video 22.1 ). The superior chest anchor line is stable. The residual skin should tightly cover the torso. Both the ptotic gynecomastia and the loose mid-torso skin are corrected with obliteration of the IMF. An appropriately sized NAC is vascularized by an inferiorly based full-thickness skin pedicle for superior translocation. The NAC is relocated into a receiving dome that lies about 3 cm superior to the inferior/lateral margin of the pectoralis major muscle. A subtle contour depression, corresponding to the lateral/inferior pectoralis muscular edge, rises from medial to lateral. This muscular adherence is roughly one interspace superior to the gynecomastia-related IMF.

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


