CHAPTER 26 Silhouette InstaLift in Men
Summary
The use of Silhouette InstaLift has become an important tool for plastic surgeons in the armamentarium of facial rejuvenation. It is a minimally invasive technique that can result in an improved appearance in appropriately selected patients. Silhouette sutures use cones to anchor, remodel, and reposition soft tissues. The on-label indication for Silhouette InstaLift is for use in midface suspension surgery (i.e., to fixate the cheek subdermis in an elevated position). However, authors have used Silhouette InstaLift in other fashions as well. Patients for whom Silhouette lift procedures are ideal are those with mild-to-moderate skin laxity in the neck and midface, malar fat ptosis, an irregular jawline, and deep nasolabial folds. This chapter will detail the indications and technique for the use of Silhouette sutures in male patients.
Introduction
The three main components of facial aging include atrophic skin change, volume loss, and ptosis of soft tissue. For the male patient, ptosis management can be challenging. This is compounded by the reluctance to accept the risk of preauricular scarring because of an inability to use hair the way women do to conceal potential scarring. As a result, the potential appeal of nonsurgical tissue redraping is very attractive.
Compared to traditional cosmetic surgical procedures, minimally invasive techniques are quick, relatively inexpensive, and associated with a shorter recovery. Outcomes can be less dramatic; however, they can result in a more natural appearance compared to more extreme open techniques. A relatively new concept in minimally invasive facial rejuvenation is the use of barbed sutures to elevate soft tissues of the face and neck. Several surgeons around the world have used a variety of sutures that differ in design, morphology, and material for this purpose. Initially, reports were varied, and there was no consensus on the optimal suture choice or technique. In 2003, the California-based plastic surgeon Nicanor Isse began using barbed polypropylene sutures for facial soft-tissue remodeling and repositioning. Early results were favorable; however, longer-term studies revealed that the physical effects of the barbs themselves may have been responsible for several complications including suture breakage, palpability, irregularity, and visibility. To avoid these, Isse designed a similar suture in which cones replaced the barbs.
The development of this novel suture—termed Silhouette sutures—has improved results and versatility with respect to minimally invasive facial rejuvenation. Silhouette sutures, which received Food and Drug Administration (FDA) approval in 2006, are composed of a 25-cm 3–0 nonabsorbable polypropylene suture and absorbable cones made of poly- L-lactic acid that are held in place by six uniformly spaced knots. Variations of this product have since been developed. The most recent, which received FDA approval 2014, is Silhouette InstaLift, which consists of a resorbable PLGA (polyglactin 910) suture with bidirectional cones. The cones are designed to lift and hold (i.e., suspend) the soft tissues through which they are passed. Furthermore, a fibrous reaction occurs around the cones to a greater extent than around barbed sutures, facilitating a stronger result. The on-label indication for Silhouette InstaLift is for use in midface suspension surgery (i.e., to fixate the cheek subdermis in an elevated position). However, authors have used Silhouette InstaLift in other fashions as well. Specific details and steps of the procedure as practically applied on- and off-label (without the use of anchoring sutures), in addition to case examples, will be provided in this chapter.
Anatomy
The goals of face-lift procedures are largely the same for males and females. However, plastic surgeons performing these procedures must be aware of several characteristics unique to the male patient. Examples include differences in aging, anatomy, and psychosocial factors. Several thorough descriptions of face and neck anatomy have been described previously (see Suggested Readings, Prendergast.). Here, we summarize facial anatomy while focusing on the key distinctions in male patients.
The primary aesthetic goal when performing any facial procedure in the heterosexual male population is often to avoid feminization of the face. Specific modifications to the technique in transgender populations are currently under study but will not be addressed specifically here. Additional considerations in male facial rejuvenation include adequate treatment of platysmal banding, volume restoration, elimination of jowling (i.e., to create a streamlined jaw), and the creation of an acute cervicomental angle. During the aging process, there is increased descent of the melolabial mound, a greater degree of midfacial hollowing, and more significantly pronounced nasolabial folds in men compared to women. In addition, men often have a heavier appearance in the neck region because of dehiscent platysmal musculature, excessive submental fat, and redundant skin. Men generally report a greater degree of concern in their neck and midface, while women are more concerned with the appearance of their upper face. Key distinctions that must be considered early in the evaluation of male patients are hairline and beard patterns.
Men can present in a variety of ways with respect to their hairline, including normal growth of hair at the temporal hairline, thinning of hair and temporal rescission, or significant male-pattern baldness. In an open face-lift, incision placement often differs depending on this pattern of temporal hair growth. However, this is less important when Silhouette or other minimally invasive techniques are used as incision placement is minimal and consistent. The presence, pattern, and color of facial hair should also be analyzed and a discussion must take place regarding how it might affect the intended procedure. Similar to the hairline, facial hair characteristics have important implications during invasive face-lifting techniques but less so during less invasive procedures. In either case, dermal injury, often the result of thermal damage, has the potential to cause alopecia and should be discussed preoperatively.
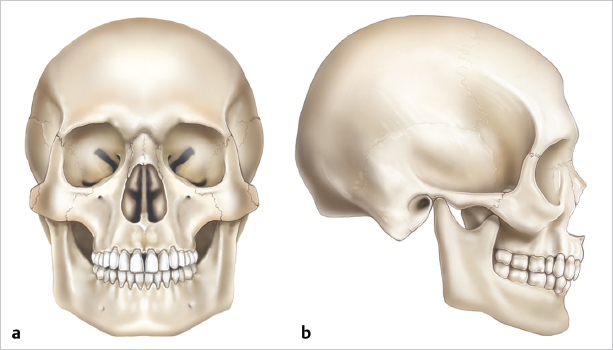
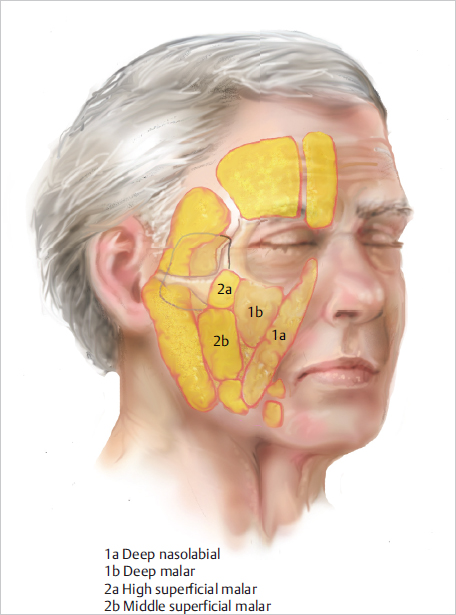
To a great extent, appearance is largely the result of the underlying facial bones and their associated convexities and concavities ( Fig. 26.1 ). Relative to females, males often demonstrate decreased projection of the zygomatic bones, increased projection of the mental protuberance of the mandible, and a larger and wider mandible. The facial skeleton provides attachment areas for the muscles of mastication and muscles of facial expression and also provides structural support and protection of the sensory organs (e.g., eyes). The face also consists of several distinct superficial fat compartments, including the superior, inferior, and lateral orbital fat pads; the medial, middle, and lateral temporal-cheek “malar” fat pads; and the central, middle, and lateral temporal-cheek pads in the forehead ( Fig. 26.2 ). These compartments are separated by the convergence of facial tissue and septae to form retaining ligaments. Retaining ligaments are classified as either true or false. True retaining ligaments connect the dermis to the underlying periosteum and are easily identifiable. Oppositely, false retaining ligaments, which connect superficial and deep fascia, are relatively diffuse condensations of fibrous tissue. When performing Silhouette lifting, it is crucial that the surgeon understands the anatomy and relationships of the retaining ligaments as subcutaneous placement has deeper tissue implications.
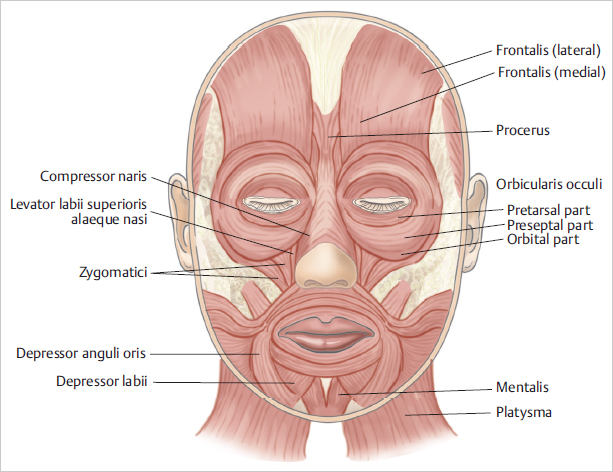
Below the superficial fat compartments are the muscles of facial expression, which can act as constrictors/ dilators of facial orifices or as elevators/ depressors of the perioral and periorbital areas ( Fig. 26.3 ). The perioral muscles include the levator, orbicularis oris, depressor anguli oris, depressor labii, mentalis, risorius, and zygomaticus major and minor. The nasal muscle group consists of the depressor septi, compressor naris, and dilator naris. Finally, the periorbital muscles are comprised of orbicularis oculi, procerus, corrugator supercilii, depressor supercilii, and frontalis. Deep to the muscles of facial expression is a deep plane that consists of deep fat compartments. These compartments facilitate gliding and moving of the muscles of facial expression as well as provide volume and shape to the face.
Described in 1976 by Mitz and Peyronie, 1 the superficial musculoaponeurotic system (SMAS) is a fibrofatty superficial fascia that lies between the muscles of facial expression and the dermis. Many invasive face-lift techniques will involve dissection, mobilization, and redraping of the SMAS. The SMAS is continuous with the platysma inferiorly, the superficial temporal fascia in the temporal area, and the galea aponeurotica superiorly. The facial nerve and its branches are located deep to the SMAS for the majority of their course ( Fig. 26.4 ).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


