CHAPTER 27 High-Definition Abdominal Liposculpture
Summary
The new concept of high-definition liposculpture is a result of the desire for belly muscular definition. New medical devices have allowed surgeons to make liposuction easier, safer, and better at producing enhanced, more desirable results. Muscular definition must be in harmony with the natural movement of the underlying muscles to provide a muscular, athletic, and natural look. Several techniques for a successful result are noted in this chapter, such as an extensive preoperative marking discussion that includes tips for “stealth incisions” and tips for dealing with the obese patient.
Introduction
Since the advent of liposuction, many improvements to the original technique have been described through medical literature. In fact, the original procedure just focused on removing adipose tissue from undesirable zones and to avoid the many different complications related to the use of possible harming instruments in the abdomen. However, since the advent of high-definition liposculpture (described by this chapter’s author), a new concept was conducted to understand the difference between a natural, slim, and athletic appearance rather than a plastic and unexpected one.
Although gym, fitness clubs, and other sport centers have done better economically in the last half-decade, because of people’s more frequent visits, a very few people have the habits, diet, and lifestyle to get the desired six-pack abs. New standards of beauty have risen in recent years, the influence of global communication and social media also influences the way that we see a fit body. That is the reason why many people do visit us at our office asking for belly muscular definition.
The use of new medical devices and technologies has allowed aesthetic surgeons to enhance results and make the liposuction procedure easier and safer, producing better outcomes. However, as each surgeon has his or her own techniques and preferable devices, there have to be some premises and features that need to be followed to get optimal postoperative effects. The muscular definition perception has to be adapted, not only by how in rest the appearance must be, but also in harmony with the natural movement of the underlying muscles. In our experience, we benefit from the advantages offered by third-generation ultrasound technology to improve the liposculpture technique in the superficial and deep approach, by facilitating the extraction of the adipose tissue, while diminishing the blood loss. The use of specific instruments and a correct technique will let us shape the body the way we want: a muscular, athletic, and natural look, like artists do with sculptures. We will try to expose in the next section how this concept has been reached and the different tips that the surgeon has to understand to perform an optimal abdominal body-contouring surgery in the male patient.
The All-or-Nothing Lipoplasty
One important goal to obtain the best results is the number of muscular groups that will be contoured. The more the muscular groups, the more natural the patient will look. If we contour only the anterior abdomen, for example, leaving the pectoral area, the oblique muscles, and the flanks untouched, the patient will look very awkward. The ideal is to perform the pectoral area, the arms, and the torso in 360° including the flanks and back to obtain the best outcomes.
Physical Evaluation
It is important to do the proper patient selection when performing these specific procedures.
Body mass index (BMI) within the normal range is ideal.
Usually, patients who are underweight might benefit from this procedure in selected cases.
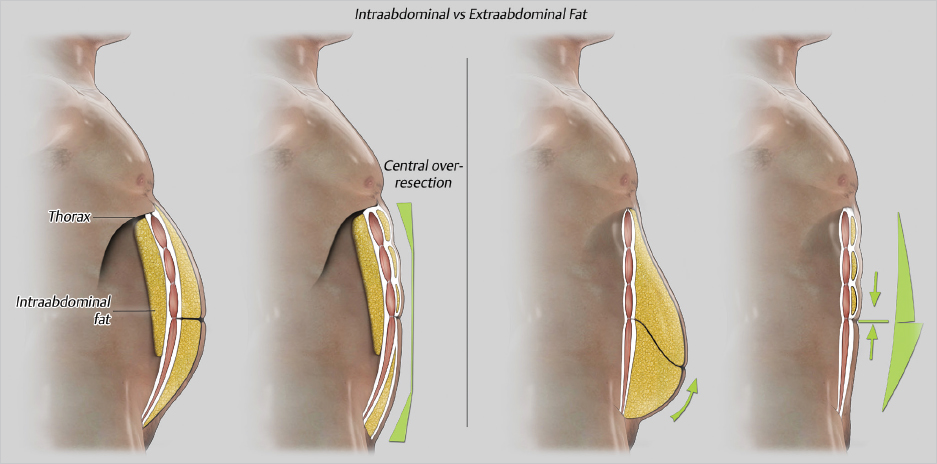
The obese patient might be a good candidate for high-definition liposuction. However, it is important to address how much of this fat, specifically in the anterior abdomen, belongs to the intra-abdominal area ( Fig. 27.1 ). These patients will need, besides surgery, proper dietary counseling to reduce the intra-abdominal fat.
Patients with previous liposuction are usually poor candidates for definition.
Patient Selection
Patients whose BMI is greater than 34.
Massive weight loss patients.
Patients who had previous bariatric surgery.
It is also important to address the presence and physical examination of the following:
Hernias.
Irregularities as a result of trauma.
Asymmetries as a result of bone structure (scoliosis, rib cage asymmetries).
Muscular deformities or asymmetries as a result of training, complexion, or overtraining (e.g., a tennis player).
Steps for High-Definition Liposculpture
Stealth Incisions
Numerous incisions are required to perform high-definition lipoplasty. Consideration must be given to the location of these incisions. As surgeons, the balance lies between operating comfortably from easy access sites that leave visible scars and hiding incisions in concealed folds or creases, at the cost of working from awkward positions that may necessitate special design of tools to reach all the areas to be contoured.
Even small incisions can leave conspicuous scars, particularly if they are hyperpigmented or hypertrophic. Various factors influence the healing process, including age, race, presence of body hair in men, and the suturing method. When closure is indicated, the author recommends subdermal continuous sutures. The ideal access points should not leave visible scars over the abdomen or the back and should be hidden in the underwear or in the natural folds of the skin. This avoids stigmata of lipoplasty surgery, such as visible or symmetric linear scars. Even with good contouring results, some patients are reluctant to wear a bikini or sunbathe if noticeable scars are present. We have to remember that the signature of the surgeon is the invisibility of the scars; the better surgeons we become, the more invisible they should be.
The author has perfected the use of hidden or “stealth” incisions. For this purpose, we developed various cannula designs to easily access the entire anatomy.
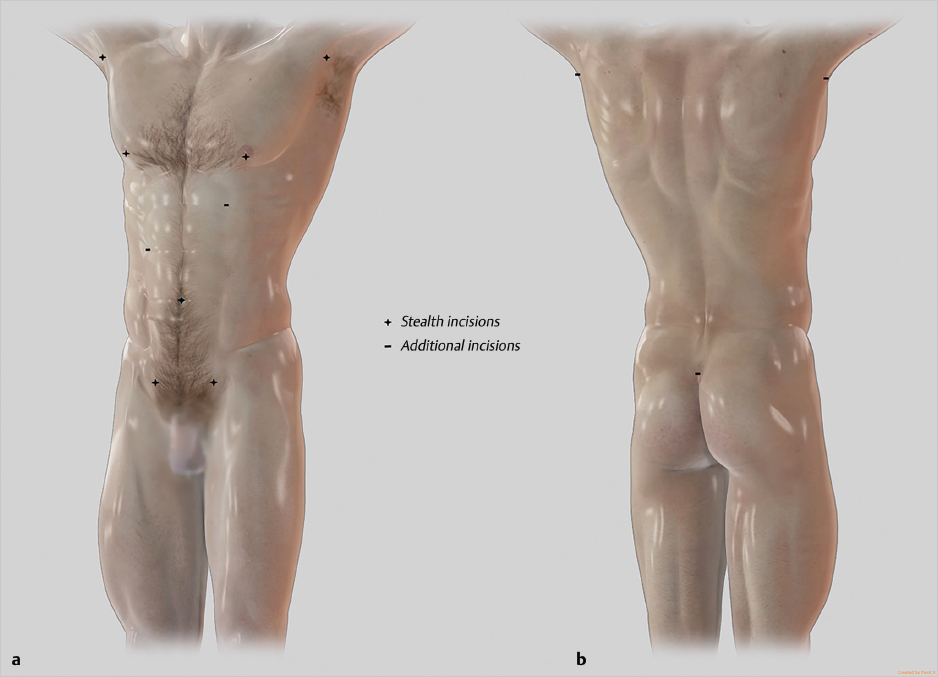
In men, the ideal incision points should be the following ( Fig. 27.2 ):
Pubis: below the hairline, two incisions in line with the semilunaris lines (lateral rectus abdominis). These provide access to most of the abdominal area, including the flanks and waistline, and the rectus abdominis bellies.
Umbilical: provides access to the inferior abdominal area, vertical midline above the umbilicus, and central supraumbilical abdomen.
Nipple crease: In men, this incision is the most hidden one, providing access to the pectoral area, the upper abdomen and the superior flank, and axillary areas.
Anterior axillary fold: provides access to the arm, pectoral area, and lateral chest. This site is essential for fat grafting in pectoralis major and minor and gynecomastia removal.
Surgical Marking
In the abdominal area, stealth incisions are always preferable. In men, it is often difficult to avoid abdominal incisions, which is preferable because they are very visible. However, if additional access sites are necessary to define the horizontal tendinous intersections of rectus abdominis, asymmetric incisions can be placed along the abdomen, ideally mimicking cholecystectomy incisions.
The preoperative markings are done in three steps with the patient in the standing position. It is recommended to use different color markers for different stages.
Deep Markings
First, the typical liposuction markings are made in the areas where extra fat is located: usually on the abdominal area, mostly infraumbilical, the “love handles,” the flanks, the pectoral area, and lateral to it toward the axilla ( Fig. 27.3 ).
Framing
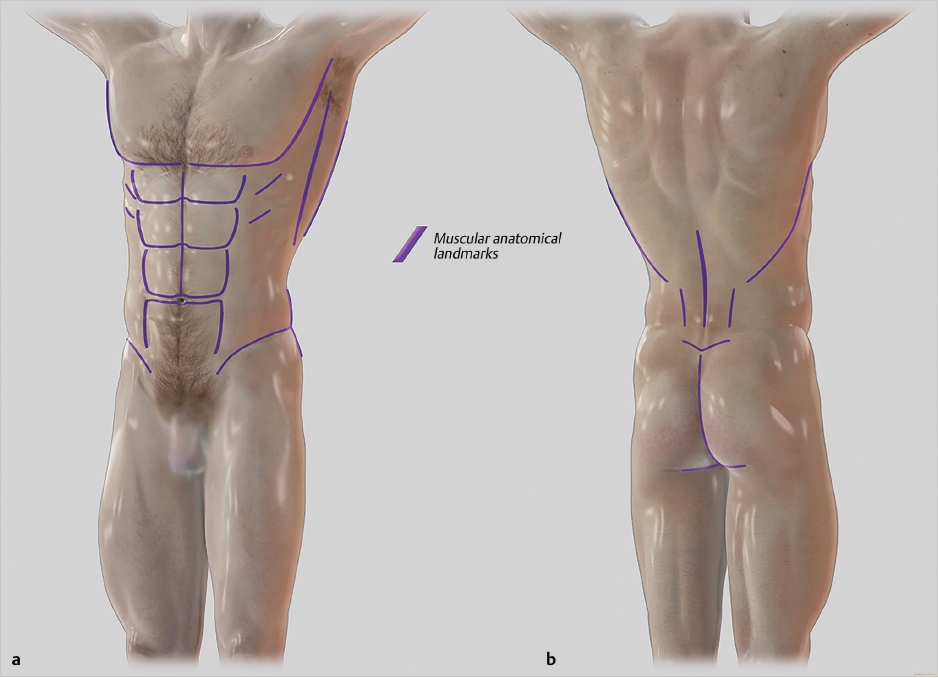
The framing is the marking that represents the actual position of the muscles and other superficial anatomical landmarks. The location of these landmarks might be defined by palpation with the patient at rest and may require the patient to contract the muscles in specific areas and positions. Sonographic guidance is particularly useful in obese patients, not only to find the muscles but also to evaluate the amount of intra-abdominal fat (which is not treatable by liposuction), so it is better to have an echography machine at hand in these cases.
The initial assessment of the position of the muscles and tone has to be done with the patient in the standing position.
Ask the patient to inhale deeply until the costal margin is visible. Mark the costal margin bilaterally to define the thoracic arch.

Palpate and mark the linea alba in the midline from the supraumbilical area to just below the xiphoid process. Remember that no midline should be marked below the umbilicus ( Fig. 27.4 ).
Feel for the lateral borders of rectus abdominis. If possible, try also to locate the transverse tendinous intersections by carefully palpating with the tips of the fingers. Ask the patient in the standing position to contract the abdominal muscles to find the grooves between the muscle bellies. This is usually possible in thin and athletic patients but may be more challenging in patients who are overweight or obese. Later we will discuss how to find them in obese patients.
Locate and mark the borders of the transverse and oblique muscles bilaterally. Ask the patient to push out the abdomen as much as possible. This maneuver reveals the shape of the muscles, particularly in patients with more intra-abdominal fat.
Sit in front of the patient at an angle of 45°, ask him to place his hand on your shoulder, and then push your shoulder downward. The large latissimus dorsi, the anterior bundles of serratus muscle, and the upper portion of the oblique muscles are easily visible and marked as they contract ( Fig. 27.4 ).
Markings in the Obese Patient
In the obese patient, marking the anterior abdomen for high definition can be challenging. There are two main scenarios in obese patients:
Predominantly intra-abdominal fat content: while this kind of patient is more challenging in terms of results, the markings are straightforward. The anatomical position of the rectus abdominis might be distorted by the intra-abdominal contents (rectus diastasis), but the position of the abdominal bellies is easy to pinpoint.
Predominantly extra-abdominal fat content: this is the most challenging patient to mark and to obtain good results. While the pectoralis markings are never a problem, excessive fat obscures the rectus abdominis landmarks. There are additional positions to mark rectus:
In the supine position, ask the patient to perform an upper abdominal crunch and mark the lateral borders of the rectus during contraction. The upper tendinous intersections are often also palpable in this position.
Next, in a sitting position, ask the patient to do a lower abdominal crunch while raising the legs. During this maneuver, the lower insertions of rectus abdominis should be palpable or even visible.
The main fat extraction in male obese patients varies according to the presence of intra-abdominal versus extra-abdominal fat. In patients with extra-abdominal fat, the resection is focused on the lower abdomen, and retraction is highly encouraged by performing thorough superficial fat resection ( Fig. 27.1 ).
In patients with mostly intra-abdominal fat, fat resection is focused more thoroughly over the central abdomen to diminish the curvature of the anterior abdomen. As the intra-abdominal fat cannot be reached by liposuction, a strict high-protein and low-carbohydrate diet after the surgery should be followed to reduce body fat.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


