CHAPTER 23 Gynecomastia: Expert Technique
Summary
After 35 years of surgical experience and having performed 8,000 gynecomastia corrections—including over 1,000 cases of severe gynecomastia with saggy breasts—I have developed a minimal incision solution to this complex problem. The traditional solution of full excision causes extensive postsurgical breast scarring and does not serve patients with severe gynecomastia well from an aesthetic point of view. It is especially ill-suited for younger men to have extensive postsurgical scars because of the chance that they may be exposed when they expose their chest at the beach, the pool, during sports, or at various social events. Most men are very discrete and will not expose their chests should their postsurgical scarring be severe. Looking at current surgical practices, I decided a practical and reasonable solution was necessary, requiring a surgical technique that does not rely on skin reduction, which almost always results in unsightly scars. My technique employs a traditional plastic surgery principle: skin defatting and undermining. This method creates large skin flaps, resulting in skin contractibility. It obliterates dead spaces, so excess skin can redrape snugly over the resulting smaller postsurgical breasts. The minimal incision surgical technique eliminates the need for extensive skin excisions, and therefore reduces scarring. The technique requires extensive surgical experience to determine the extent of the undermining and deflating, and the more I use this innovative technique, the more impressive my surgical outcomes have become. The minimal incision technique is a nuanced approach and does not provide as quick a result as simply cutting out the skin—but the results are much more natural. It is of paramount importance to discuss this with patients, to encourage patience, and to reserve judgment until the final results. Only a small percentage of severe patients will need a secondary surgery. The minimal incision surgical technique has proven extremely useful with very high patient satisfaction rates.
Introduction
Many surgeons finish their residency and fellowship training with little exposure to gynecomastia surgery and have questions regarding how to approach the more severe gynecomastia patients who have excess skin and breast ptosis. When beginning to treat gynecomastia patients, as with many other surgical techniques, there is a learning curve and the less experienced surgeon might consider starting with less challenging cases and working toward more complex patients.
The senior surgeon’s operative technique adheres to several surgical principles, which include the following: He has performed over 8,000 gynecomastia cases over the past 30 years, with high patient satisfaction in a competitive geographic area.
Minimal inferior areolar incisions place more laterally.
No skin excision.
Concomitant liposuction.
Obliteration of the inframammary fold with undermining.
Near complete excision of breast glandular tissue.
Our technique contradicts traditional surgical treatments for severe gynecomastia, where excess skin is excised through a lengthy incision. Many gynecomastia patients who seek surgical treatment have kept themselves covered for many years and desire the freedom to go without a shirt and to wear whatever they like. We believe that traditional surgical techniques, which often result in a long scar, defeat the purpose of the surgery whereby they trade a contour problem related to gynecomastia for a scar problem, which most patients want to avoid. Gynecomastia surgery should avoid the commonly used skin patterns and incisions used in female breast surgery. By keeping incisions small, patient satisfaction remains high. We favor minimal subareolar incisions with wide undermining and skin redistribution, over excising excess skin in even the most severe gynecomastia patients.
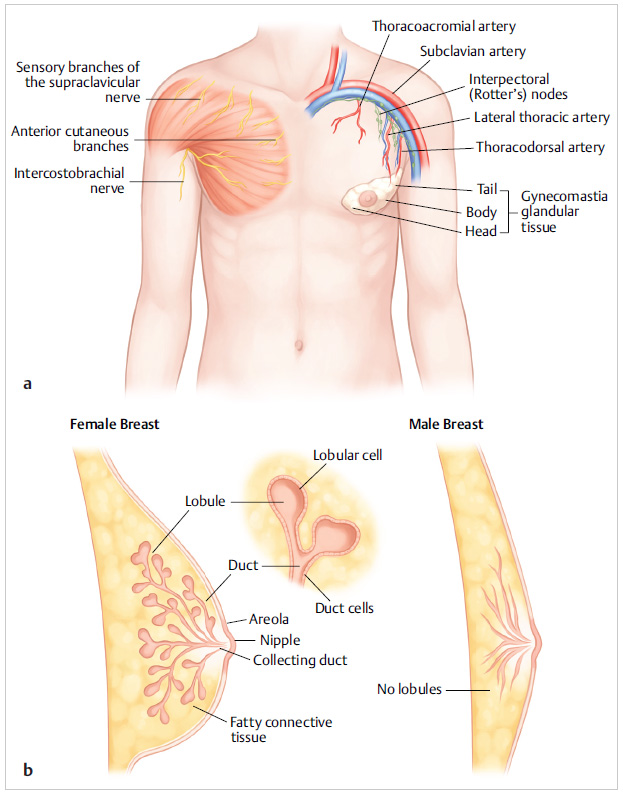
In our experience, gynecomastia patients desire a flat chest contour with accentuation of the underlying pectoralis major muscle. Patients with gynecomastia tend to have a more pyramidal breast shape, mimicking a female breast appearance. From an anatomical point of view, the male and female breasts have similarities. Breasts in both men and women extend from the second to sixth anterior ribs with the sternum as the medial border and midaxillary line demarking the lateral border ( Fig. 23.1a ). Men typically have predominantly fatty tissue with fewer ducts and stroma, whereas ducts, stroma, and glandular tissue predominate in women’s breasts. Unlike the female breast, the male breast lacks lobules, and therefore has no mammary secretions ( Fig. 23.1b ).
Patient Presentation
Gynecomastia is prevalent and has been reported to affect nearly 50% to 70% of the male population. Patients are interested in gynecomastia surgery for several different reasons. Bodybuilders generally present complaining of excess breast tissue that interferes with their desired physique and affects their professional level at competitions. Many other patients, who are not professional athletes, present complaining that their breasts appear “more female-like,” which makes them self-conscious in social situations both with and without a shirt (i.e., going swimming, when performing water sports, when intimate with their partners). Patients often complain that they avoid removing their shirt in public and maintain a hunched posture to hide their breast silhouette. Many teenagers and children present with their parents because of being bullied and teased at school. They report feelings of shame and isolation. School-aged patients may also try to avoid sport activities, which may interfere with their self-confidence and social integration.
Steps of Procedure: Gynecomastia
Preoperative Preparation
Thorough preoperative preparation is of utmost importance. We have extensive discussions with our patients and do our best to set realistic patient expectations. Surgical outcome depends on many factors such as patient age, weight fluctuations, skin elasticity, and severity of gynecomastia including skin excess and breast ptosis.
Consent is obtained for gynecomastia surgery with major risks discussed, which include but are not limited to infection, bleeding, scarring, asymmetry, need for further surgery, seroma, hematoma, possible persistent skin excess, and contour deformity. In those patients with severe gynecomastia who have inelastic skin because of age or inherent skin quality, the patient is counseled that although rare, reoperation may be required. Often the patient accepts a small degree of skin excess over the risk of having a long incision.
As with many other plastic surgical procedures, our patients undergo routine preoperative clearance. Those patients with medical problems require more extensive preoperative workup, especially patients with diabetes or any cardiac history. Diabetic patients require strict blood sugar control. Because extensive undermining may be performed, patients must stop smoking a minimum of 6 to 8 weeks before and after surgery. Weight loss is encouraged preoperatively to decrease surgical risk and possibly to improve chest and abdominal contour postoperatively. Bodybuilders may be taking fish oil or steroid supplements, which are stopped preoperatively to decrease the risk of bleeding and help improve wound healing.
Patient Markings
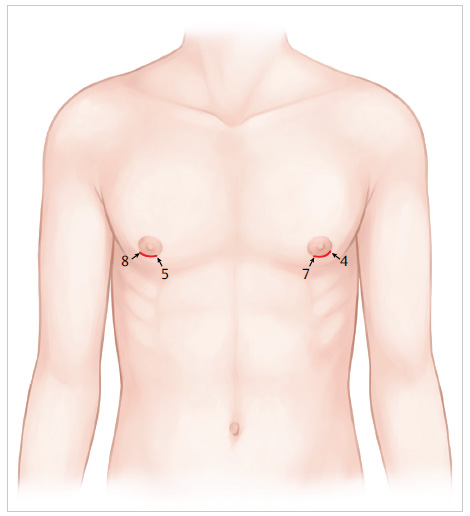
The patient is marked in the preoperative area in a standing position. Incisions are planned along the lateral inferior areolar border. The senior surgeon feels the scar is more hidden when placed along the lateral aspect of the inferior areola. Over time, we have moved the inferior areolar incision more laterally, which has improved patient satisfaction. Circumareolar incisions are never performed; we avoid these incisions even in extreme cases. On the right side, the incision is marked from the 5 to 8 o’clock position; on the left side, the incision is marked from the 4 to 7 o’clock position. Incisions are approximately 2 to 3 cm in length in most cases ( Fig. 23.2 ).
The glandular area to be excised is then marked, including any axillary glandular tissue, which results in a circular or oval marking pattern. Care must be taken to outline the entire area of glandular tissue to be excised. The inframammary folds are clearly marked bilaterally. Areas to be liposuctioned are then outlined, which include the periglandular tissue, and may include the axillary and superior abdominal area in patients with thicker subcutaneous fat in those regions. Areas to be undermined are marked next, which include the area overlying the sternum across the midline, inferior through the inframammary folds, and possible extension inferiorly in those patients with severe gynecomastia.
Surgical Procedure
The majority of our procedures are performed under intravenous sedation in the supine position in our accredited outpatient office-based operating room. The patient’s arms are placed with adequate padding at the patient’s sides. After intravenous antibiotics are provided, the patient is prepped from the suprasternal area to the umbilicus. Lidocaine 0.5% with 1:200,000 epinephrine mixed with 500 mL of normal saline is instilled with a long spinal needle (18 gauge, 3.5 inches long) on a 60-mL Luer-Lock syringe to all planned surgical sites, which include the glandular tissue to be excised, as well as regions to be liposuctioned and undermined. Between 200 and 500 mL of tumescent is generally used, with the higher range reserved for more severe gynecomastia and larger patients.
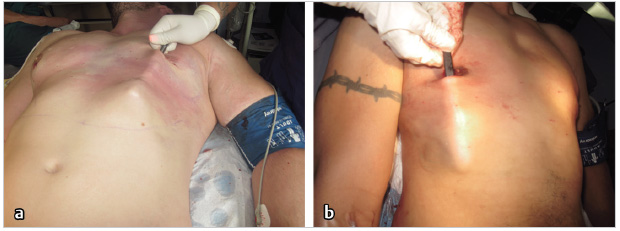
Liposuction is then performed through 3-mm stab incisions along the inferior areolae, which will be incorporated in the ultimate skin incision. A 3-, 4-, or 5-mm Mercedes tip liposuction cannula is used. Liposuction is most frequently performed with power-assisted liposuction (MicroAire). When a liposuction machine is not available, liposuction using syringe aspiration has been successfully performed, even in those patients with severe gynecomastia. Liposuction is generally performed in the periglandular area but may extend into the axillary and superior abdominal areas as needed ( Fig. 23.3 ).
After liposuction is performed, incisions are made with a No. 15 blade and deepened with electrocautery. The inferior areolar incision extends more laterally than medially ( Fig. 23.2 ). The glandular tissue is then excised en bloc. Near complete glandular tissue is performed in all patients ( Fig. 23.1a,b ). In bodybuilders and very athletic patients, approximately 2 to 3 mm of subareolar glandular tissue is left behind. In other patients, including slightly overweight patients, approximately 5 mm of subareolar glandular tissue remains ( Fig. 23.4 ). If more tissue is taken in these patients, they may have contour depression or “dish saucer deformity,” since they have a greater amount of surrounding adipose tissue. Glandular tissue is excised using a combination of cautery and direct excision with face-lift scissors. Care must be taken to remain superficial to the pectoralis fascia at all times, as we believe this helps to decrease the risk of seroma and hematoma. Excised glandular tissue is always sent to pathology for evaluation, even in cosmetic cases. Although rare, the senior surgeon has found cancer in some glandular specimens.
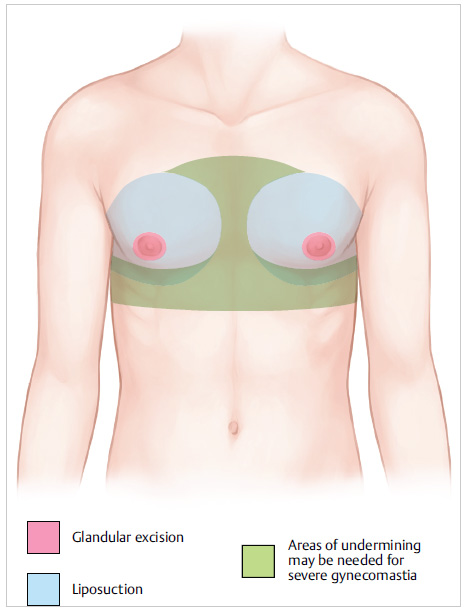
Skin flaps are then raised and undermining performed with face-lift scissors. Hemostasis is achieved with electrocautery while undermining. Undermining is always performed from the inferior areolar incisions directing the scissors inferiorly beyond the inframammary folds into the upper abdominal area. Undermining extends inferiorly beyond the inframammary fold to obliterate the feminizing inframammary fold and allow the excess breast skin to descend and contract ( Fig. 23.5 ). This maneuver almost universally results in some flattening of the inframammary fold, which is desired by gynecomastia patients. To enhance skin contractility after surgery, excess subcutaneous tissue is excised leaving skin flaps with a uniform thickness of approximately 3 to 5 mm. The resultant skin flaps created with our technique are similar to those created with nipple–areolar skin-sparing mastectomy. In patients with skin excess, undermining may be extended across the midline and inferiorly to the umbilicus ( Fig. 23.3 , Fig. 23.6 ). Undermining to the axillary area is sometimes performed in patients with skin excess in that region, but this is performed less frequently. In this way, extensive undermining takes advantage of the skin’s inherent elastic and contractile properties to shrink and evenly redistribute across the chest and upper abdomen, in even the most severe gynecomastia cases with significant skin excess ( Fig. 23.3 ).

According to the senior surgeon, several “tissue types” are encountered in this procedure. In younger patients and bodybuilders, the glandular tissue is very well circumscribed and essentially impossible to liposuction. These patients may have fatty tissue surrounding the gland that can be liposuctioned. In older patients, the glandular tissue transitions more gradually to the surrounding areas, with a greater proportion of fat in the glandular tissue, which enables some amount of liposuction at the periphery of the gland and surrounding areas. Just as in female patients, the glandular tissue may have a higher proportion of fat with increased age and weight of the patient.

Medial undermining across the midline is performed in patients with very severe gynecomastia. The need for this is assessed after the inframammary dissection is completed. In contradiction to traditional principles of breast surgery in females, where medial dissection over the sternum is avoided to prevent synmastia, in gynecomastia surgery, complete undermining across the sternum may improve the medial breast contour. Medial undermining is performed with electrocautery and face-lift scissors, with care to avoid the internal mammary perforators by using blunt dissection in line with the perforators. Particular attention must be paid to cauterizing this area to ensure adequate hemostasis. Similarly, lateral dissection should avoid the lateral thoracic perforators by dissecting in line with them ( Fig. 23.3 , Fig. 23.4 ).
By following the basic principles of plastic surgery related to skin elasticity and contractility, we achieve excellent contour while keeping incisions and resultant scarring to a minimum. Our patients have expressed that their scars are inconspicuous ( Fig. 23.7 ). The undermined skin and inframammary folds redistribute more evenly over the chest wall, and ultimately contract and redrape over the pectoralis major muscles and superior abdominal wall, highlighting the anatomy the patient desires. We have experienced excellent skin retraction with wide undermining and cautious defatting of the skin flaps. Skin flap ischemia is rarely encountered. The senior surgeon has never encountered necrosis of the areola. Epithelial sloughing has sometimes been encountered and treated conservatively.
There is a learning curve with this procedure. The amount of liposuction and undermining varies with the patient’s anatomy and severity of gynecomastia. For example, additional undermining may be needed in patients with severe gynecomastia. The patient is placed in the sitting position intraoperatively, whereby the appearance of the chest and upper abdomen is assessed, and additional undermining and tissue release are performed as needed.
In the senior surgeon’s experience, laser liposuction and ultrasound liposuction have little effect on glandular tissue. He or she also believes that laser liposuction has limited effect in patients with severe skin ptosis as compared to extensive undermining and flap defatting.
A drain is placed in approximately 2% of cases and is reserved for patients with more extensive undermining. A 1/4-inch Penrose drain or a small Jackson–Pratt drain may be used in these instances. The drain may be placed through the lateral portion of the inferior areolar incision or through a separate small axillary incision. Drains are generally removed within approximately 72 hours.
Inferior areolar incisions are closed with dissolvable sutures. With deeper interrupted intradermal buried 3–0 or 4–0 Monocryl sutures in those patients with thicker skin and superficial 4–0 or 5–0 Chromic running sutures in all patients. Bacitracin may be applied. Compression dressing with 4 × 4 fluffs, ABD pads, and Coban is placed.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


