CHAPTER 24 Gynecomastia Removal with Radiofrequency-Assisted Technology
Summary
Gynecomastia removal with radiofrequency-assisted technology has created new opportunities for a minimally invasive approach to male breast reduction. This chapter will educate the reader on appropriate patient selection, pertinent anatomy, and the new technology of bipolar radiofrequency and its uses for skin tightening and contraction. Radiofrequency-assisted lipolysis is described in this chapter as a tool to aid in the improvement of the male breast shape with a clearly delineated protocol and procedure. The risks, benefits, and alternatives to this type of gynecomastia reduction are also discussed in depth.
Introduction
Gynecomastia is the most common breast condition in men and is defined by the benign proliferation of glandular tissue in the male breast, commonly in association with excessive subareolar fatty deposits. This condition is very common, affecting approximately one-third of all men, and nearly two-thirds of boys in adolescence. Etiology of the condition is multifactorial and can be caused via various medications and drugs, but most commonly is associated with an absolute or relative excess of circulating estrogens or an enhanced sensitivity of the breast tissue to estrogen.
Initially, one must observe an appropriate interval of observation, generally 1 year minimum from onset, and a thorough medical history and examination to rule out physiological and pathological causes such as medication-induced, hormone-producing tumors, liver disease, Klinefelter’s syndrome, hypogonadism, male breast cancer, illicit drugs, and environmental factors. Once the gynecomastia is determined to be idiopathic, the most common cause, the treatment mainstay has historically been excisional techniques. These techniques were then supplanted by less invasive options such as suction lipectomy and were further enhanced with the advent of power-assisted liposuction (PAL) and ultrasound-assisted liposuction, which increased the skin contraction possible after minimally invasive removal of fatty breast deposits. Recently, with the advent of radiofrequency-assisted lipolysis (RFAL) devices like BodyTite (Invasix Yokneam, Israel), there has been a further increase in the number and type of cases that can be treated with minimally invasive techniques because of the increased soft-tissue contraction and improvement in skin laxity that can be obtained with bipolar radiofrequency.
Physical Evaluation
A complete history and physical examination are most important. Ensure the patient is generally healthy and appropriate to undergo elective surgery. In addition, the following should be evaluated:
Ask about a family history of breast cancer, especially male breast cancer.
Ensure the patient is a nonsmoker or smoke-free for a minimum of 4 to 6 weeks.
Ensure the patient has an appropriate understanding that gynecomastia reduction is a sculpting procedure, not a weight loss surgery.
Obtaining a complete history and documentation of all medications and usage of any illicit drugs is tantamount as well as the time frame of disease onset and length of disease.
Complete a thorough breast examination. Ensure there are no discrete firm masses outside the subareolar glandular tissue that could be concerning for male breast cancer and would require further work-up. Mammography may be indicated.
Examine the breast for fatty versus glandular predominance as well as unilateral versus bilateral disease, degree of ptosis, and degree of skin excess.
Complete a testicular examination to rule out hypogonadism or any mass.
Staging the extent of the disease is an important step in determining the appropriate operative course. Consider using Rohrich et al.’s classification1:
Recommended Staging for Gynecomastia
Grade I: Minimal hypertrophy (<250 g) with no ptosis.
Primarily glandular.
Primarily fibrous.
Grade II: Moderate hypertrophy (250–500 g) with no ptosis.
Primarily glandular.
Primarily fibrous.
Grade III: Severe hypertrophy (>500 g) with grade I ptosis.
Grade IV: Severe hypertrophy (>500 g) with grade II or III ptosis.
Identify any dermal striae and show the patient that these will not resolve with the procedure and are indicators of more dermal quality, which may impact the degree of skin tightening possible.
Identify the size of the nipple–areolar complex (NAC), and if it is excessively large, confirm for the patient that this procedure will not meaningfully reduce the size.
Anatomy
The anatomy of the male breast is similar to that of the female breast in terms of base footprint. The breast extends from the second to sixth ribs and is bordered medially by the lateral aspect of the sternum and laterally by the anterior axillary line. The healthy male chest is generally flat with an accentuated pectoralis major and minimal fatty tissue or ducts and stroma (Chapter 23, Fig. 23.1).
Ideal male nipple position is along or lateral to the midclavicular line and generally found along the lateral border of the pectoralis major. The nipple is ideally 1 to 2 cm above the inframammary fold (IMF) (along the fourth or fifth intercostal space). The male IMF is much less distinct than the female counterpoint and should be more of a gentle indentation defining the pectoralis musculature, ascending laterally toward the axilla from the midclavicular line. The male nipple is ideally slightly oblong and 20 to 25 mm in diameter.
The breast examination should also establish the subtype of hypertrophy present, whether more stromal and glandular in nature (florid) or more fibrous and fatty.
Steps for Radiofrequency-Assisted Lipolysis (BodyTite) for Treatment of Gynecomastia
The procedure may be performed under general anesthesia or local anesthesia with oral sedation. Most commonly in my practice, this procedure is performed under oral medication and local anesthesia with wetting solution alone.
The patients are marked standing in the preoperative holding area marking the sternal midline, the IMF, the lateral border of the pectoralis major, and the transition zone between the chest where fullness is desired (upper pectoral region) and the lower half of the chest where a flatter contour is desired.
The standard protocol is 500 mg cephalexin, one tablet of oxycodone/acetaminophen 5/325 mg, and 10 mg diazepam 30 minutes prior to surgery. The patient is placed in the supine position and prepped in the standard fashion.
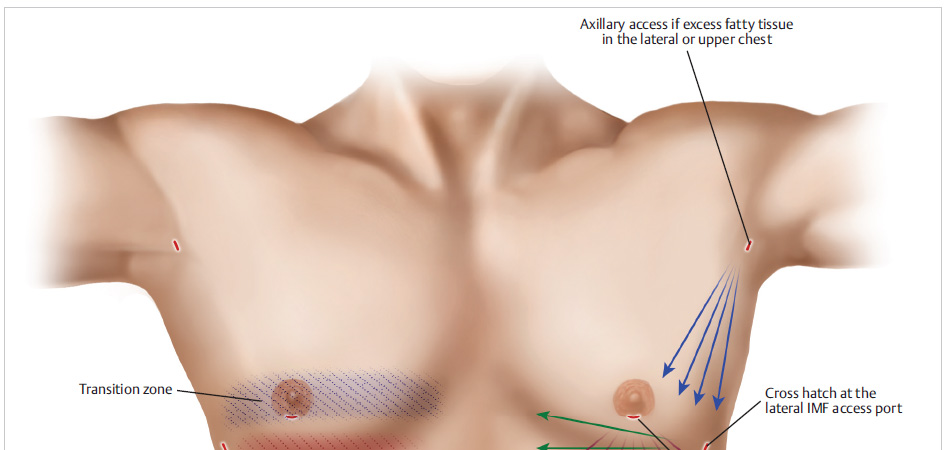
Two entry points are utilized at a minimum with the possible addition of a third depending on the degree of excess tissue and the location of the fatty deposits ( Fig. 24.1 ). The first two points are marked along the lateral border of the IMF at the inferolateral aspect of the pectoralis major insertion. The second is marked at the 6 o’clock position along the inferior border of the areola. The third, if needed, is placed hidden in the axilla at the upper outer border of the chest along the anterior axillary line.
A 30-g needle is utilized with 1% lidocaine and 1:100,000 epinephrine and is used to place a small amount of local anesthesia to the two stab incision points starting deep in the subcutaneous space and ending in an intradermal wheel. Then a No. 11 blade is utilized to create the 4-mm incisions necessary for introduction of the RFAL and liposuction cannulas.
For the awake patient, specialized wetting solution, as described by Theodorou and Chia3 of 1,000 mg lidocaine with 1.5 mL epinephrine and 10 mL sodium bicarbonate in 1 L of Ringer’s lactate is used. The rate of infusion should be kept slow and steady to allow the most painless infusion possible for the patient. Generally, 300 to 500 cc of fluid are used per side.
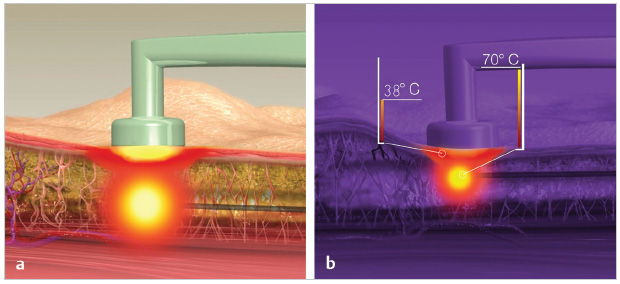
We utilize the FaceTite handpiece most commonly for gynecomastia as it is smaller and easier to handle than the larger handpiece ( Fig. 24.2 ). Settings are generally 38°C for the skin and 65 to 70°C internal. We start at the areolar incision and treat across the IMF to ensure maximal disruption of the fold and maximal treatment and tightening of the lower pole of the breast. Once the lower pole has been treated from a radial approach to the nipple, the handpiece is transferred to the lateral port, and a cross-hatching approach is taken. This allows additional heat to be delivered as well as heat across the central chest and NAC region ( Fig. 24.3 ). The aim is to treat the entire goal area at target temperature for 30 seconds to 1 minute to ensure maximal contraction of the skin and fibroseptal network below.
If there is excess fatty tissue in the lateral or upper chest, the third port site can be utilized to create RFAL to the lateral outer chest region. Be cautious not to overtreat the upper pole of the breast in the midclavicular line, as this could cause elevation of the NAC, which is not desirable in the male breast.
Once the entire region has been brought to target temperature, 4-mm cannulas are utilized for residual fat removal, focusing on the lower pole and continuing to disrupt the IMF as much as possible.

If there is any concern for step-off of the fatty tissue from the upper chest to the lower chest, or if there is concern for residual tightness of the IMF, PAL (MicroAire, Charlottesville, VA) 4-mm exploded-tip cannulas off-suction can be utilized to disrupt the fold further and smooth out contour deformities or step-offs with some fat redistribution.
This technique, which allows for skin retraction of up to 33%, is likely to avoid excisional techniques of any skin.2 However, it is important to critically analyze the on-table result, specifically for any residual stromal elements in the subareolar region. While RFAL will continue to tighten the skin and underlying tissue for months, if there is residual breast parenchyma below the NAC, this will not resolve on its own.
For residual glandular elements, an inferior periareolar incision is made, incorporating the original stab incision for the introduction of the RFAL handpiece. The incision extends from the 3 to 9 o’clock position, and with the aid of double hooks, all of the glandular elements can be resected from this access. Face-lift scissors are utilized to resect the tissue from the undersurface of the NAC, taking care to leave 1 cm of tissue deep to the NAC to ensure the avoidance of the “stuck on” nipple appearance. Grasping the gland with an Allis clamp, a combination of electrocautery and scissor dissection will allow for rapid and complete removal of remaining stromal elements.
Once meticulous hemostasis is ensured, placement of a penrose can be placed and brought out through the axillary port utilized for RFAL.
The periareolar incision is closed in the deep layer of the superficial fascial system with 3–0 Vicryl. Deep dermal and subcuticular closure are performed with 3–0 and 4–0 Monocryl suture, respectively. Steri- Strips are applied along the incision. TopiFoam and a chest binder are then placed.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


