Flap |
|
Tissue |
Fasciocutaneous/osteocutaneous flap, non–hair-bearing, can also be de-epithelialized as a pedicle or free subcutaneous fascial flap |
Course of the vessels |
Parallel to the skin above the deep fascia |
Dimensions |
Parascapular flap, 8–10 × 20–25 cm; scapular flap, 10–15 × 12–25 cm |
Extensions and combinations |
Fascial extensions; any combination with other flaps from the subscapular system |
Anatomy |
|
Neurovascular pedicle |
— |
Artery |
Constant branch of the circumflex scapular artery; vertical branch for parascapular flap; horizontal branch for scapular flap |
Veins |
Two concomitant veins |
Length and arc of rotation |
6–10 cm |
Diameter |
Artery, 1.5–3 mm; veins, 2–4 mm |
Nerve |
No sensory nerve |
Surgical technique |
|
Preoperative examination and markings |
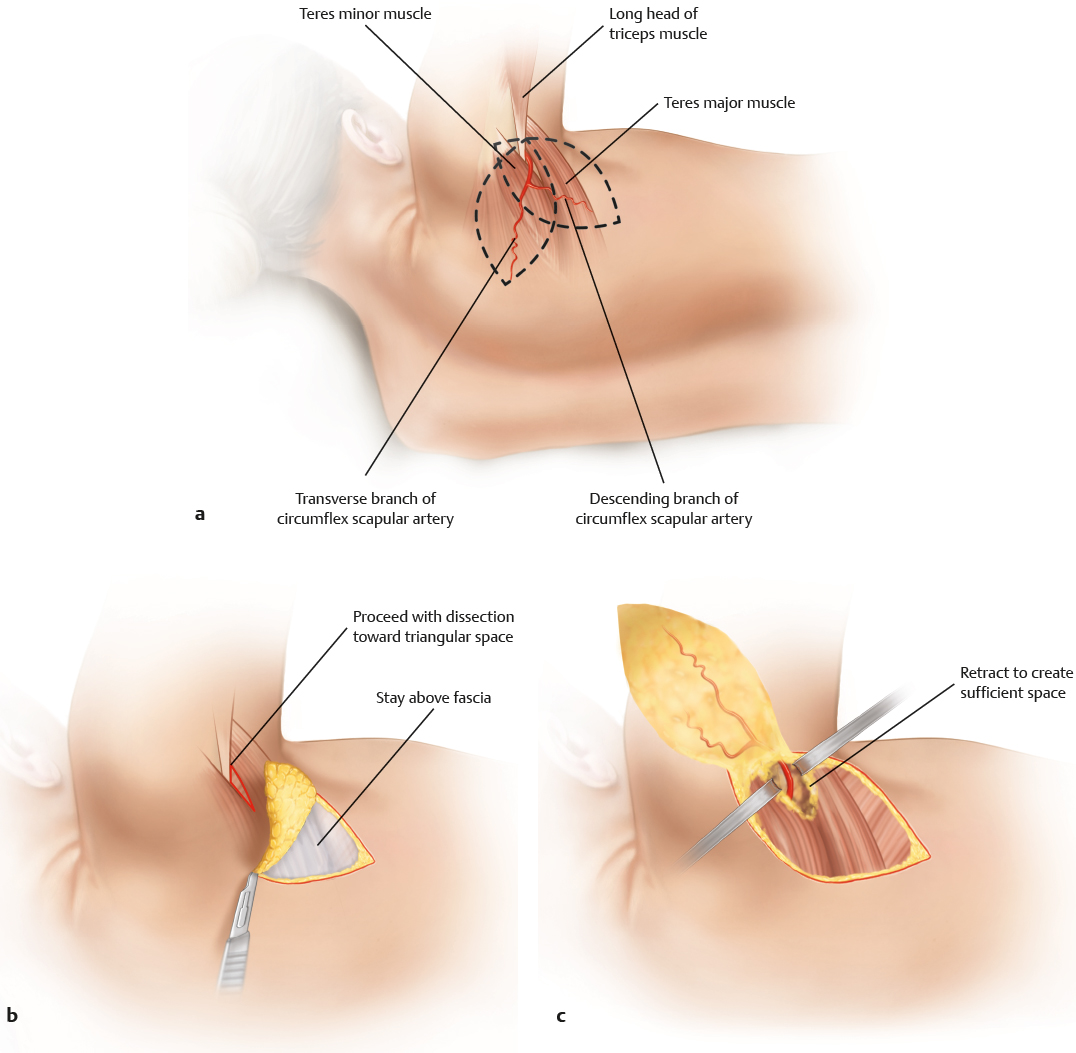
Doppler identification of vessels (horizontal and descending branch), identification and marking of triangular space (defined by teres major, teres minor, and long head of the triceps), tip of the scapula, scapular spine, spine, and border of latissimus dorsi muscle |
Patient position |
Midlateral or oblique prone position |
Dissection |
Parascapular flap: start with a low medial incision (retrograde elevation); identify the epifascial plane; proceed cranially to the area of the triangular space; complete the skin incision; identify the fatty tissue around the pedicle; carefully retract the flap medially; ligate or clip the muscle and bone branches very carefully; follow the pedicle into the triangular space; identify the thoracodorsal or subscapular artery; check for flap perfusion; perform pedicle transection or flap transfer; some authors favor the identification of the vascular pedicle as the first step of the dissection
Scapular flap: employ the same strategy of dissection as for the parascapular flap, then dissect medially and proceed toward the triangular space; as with the parascapular flap, the vascular pedicle can also be identified first during the course of the dissection |
Advantages |
|
Vascular pedicle |
Long; reliable; large caliber; arc of rotation as a pedicle flap reaches the axillary fold and the dorsal brachium |
Flap size and shape |
Large flaps possible with medial and lateral extensions and scapular fascial extension; uniform thickness of flap; can also be used as a “buried flap” when de-epithelialized |
Combinations |
Possible with all flaps from the subscapular system; very valuable: combination with bone parts for segmental forearm defects; bone segments can be harvested medially and laterally |
Further options |
Preserves most of the other flaps from the subscapular system |
Disadvantages |
|
Bulkiness |
Thickness depends on the patient’s body habitus; sometimes it is too bulky |
Donor site morbidity |
No functional loss; conspicuous scarring when scar widens; only donor sites 8–12 cm wide can be closed primarily |
Pearls and pitfalls |
|
Dissection |
Watch out for fatty tissue around the pedicle; put some stay sutures in for careful flap retraction; do not sever the large bony/muscular branch, which comes very soon after the pedicle dives deep; have the patient deeply relaxed during the pedicle dissection, which facilitates dissection into the axilla; use long blade retractors to open the triangular space |
Extensions and combinations |
Most combined flaps can be raised without altering patient position; do not violate the bony/muscular branch when taking a bone segment; include a muscle cuff; an axillary incision is only required when the flap is combined with other flaps from the subscapular system; in the case of combined flaps, do not transect the pedicle before anatomical variations have been excluded |
Contouring and correction |
May be necessary, as the flap tends to sag; debulking may be required; liposuction can be difficult due to the structure of the dorsal fatty tissue |
Clinical applications |
Resurfacing of forearm and dorsum of the hand; provision of skin coverage and gliding tissue for flexor and extensor tendons, when the fascial extension is included; perfect for segmental defects of the forearm; defects of the shoulder area and the dorsal brachium when used as a pedicle flap |