Approximately 10% of the island population of Satowan (population, 650 persons), a small, remote coral island in the central Pacific, suffers from an acquired, chronic, disfiguring skin condition known locally as “spam.” This skin disease has affected the island population since shortly after World War II. An investigation in 2007 revealed that this skin disease is caused by a nontuberculous mycobacterial infection closely related to Mycobacterium marinum . This article reviews the fascinating history of this skin disease on Satowan, its distinctive clinical presentation, and recommendations for diagnosis and treatment of clinically similar skin lesions in Pacific Islanders.
Approximately 10% of the island population of Satowan (population, 650 persons), a small, remote coral island in the central Pacific, suffers from an acquired, chronic, disfiguring skin condition known locally as “spam.” This skin disease has affected the island population since shortly after World War II. An investigation in 2007 revealed that this skin disease is caused by a nontuberculous mycobacterial infection (NTM) closely related to Mycobacterium marinum . This article reviews the fascinating history of this skin disease on Satowan, its distinctive clinical presentation, and recommendations for diagnosis and treatment of clinically similar skin lesions in Pacific Islanders.
Geography and history of the island
Satowan is one of the 607 islands in the Federated States of Micronesia (FSM), an independent, sovereign nation that extends 1800 miles (2900 km) across the Caroline Islands in the central Pacific, east of the Philippines and south of Guam. FSM comprises the four states of Kosrae, Pohnpei, Chuuk and Yap. Our story takes place in a sparsely populated, outer island cluster of atolls in the southeastern part of Chuuk, known as the Mortlock Islands. Satowan is the main islet of Satowan Atoll, one of four atolls in the Mortlocks. Two hundred miles from Chuuk’s population center in Weno, the indigenous Micronesians of the 1.1-km 2 island of Satowan have survived for centuries, living mostly a subsistence lifestyle with a diet composed of local marine life and the bounty of crops brought by their voyaging ancestors. These introduced plants provide the staple foods of breadfruit, coconut, and taro.
The Caroline Islands were likely settled by people originating from Southeast Asia around 3000 bc . In the sixteenth century, Magellan and subsequent Spanish explorers claimed this part of the Pacific Ocean for Spain, but most of these remote islands were largely ignored by the outside world until the nineteeenth century when they were visited by whalers, traders, and missionaries from Europe, the United States, and Japan. In 1898, the Spanish empire collapsed and Germany purchased many of Spain’s holdings in Micronesia. Germany had economic goals and developed local resources of copra (dried coconut meat) and guano (accumulated droppings of seabirds, from which commercial phosphates were extracted). Although claimed by European nations for more than 300 years, the central Pacific islands remained, for all practical purposes, uncolonized. That changed in October of 1914, when Japan seized Palau, Saipan, Pohnpei, Kosrae, Chuuk, and Yap from Germany at the beginning of World War I. Unlike Spain and Germany, whose interests in the islands were largely economic, Japan looked at them as an integral part of a growing empire. In addition to investing resources into roads, harbors, communications systems, and transportation facilities, Japan encouraged its citizens to colonize the islands. From 1920 to 1942, the population of Japanese living on the islands of the central Pacific grew from approximately 3000 to over 93,000. Although half of these colonial Japanese were on Saipan, by 1942 there were nearly 5000 living in Chuuk as well.
Along with the influx of Japanese families came an influx of Japanese culture. Japanese-style homes and markets were built and traditional island agriculture was replaced by Japanese crops and domesticated animals. One of the hindrances to living on these tropical islands was the abundance of mosquitoes, which bred in pools of fresh and brackish water. To counter the mosquitoes, the Japanese introduced small fresh water fish called medaka ( Oryzias latipes ) to many islands, including Satowan. Surviving in small collections of standing water, medaka ate mosquito larvae and helped control local mosquito populations (Kino S. Ruben, Medical Officer, Chuuk Department of Health, personal communication, June 2007).
In the years leading up to World War II, Japan’s intentions in the region shifted from economic development and colonization to military transformation as they established military bases throughout the central Pacific. Chuuk’s main population center in Chuuk Lagoon (then known as Truk Lagoon) comprises a tight cluster of high volcanic islands surrounded by a 50-km wide lagoon that, in turn, is surrounded by a circumferential, halo-like protective coral reef. This unique geography made Truk Lagoon an ideal maritime stronghold for the Japanese fleet. Known as the Fourth Base Force ( konkyochitai ), Truk soon became the forward anchorage for all Japanese naval garrisons in the Eastern Caroline Islands. Smaller, outer islands were also used by the Japanese military. As the widest strip of land in the Mortlock Islands, Satowan was an ideal location for a small, remote airbase. Construction began in 1943 after residents of Satowan were forced to move to Kutu and Moch, two smaller islets on Satowan Atoll. A concrete runway and other military installations were built, transforming Satowan into Japan’s largest military base in the Mortlock Islands.
On February 17, 1944, a United States carrier fleet began a now historic 2-day bombing of Truk Lagoon in a mission known as Operation Hailstone. Forty-five Japanese ships and 275 Japanese aircraft were destroyed and another 27 vessels were damaged, essentially removing Truk lagoon as a major threat to Allied island-hopping operations in the central Pacific. Allied forces then disabled Japanese installations elsewhere in the Carolines and reclaimed control of the central Pacific. Nevertheless on April 30, 1944, eight US destroyers and nine cruisers bombarded Satowan with 1400 rounds of 5-inch shells and 800 rounds of 8-inch shells, destroying the runway and surrounding military installations. Although the bombardment met with no opposition and is described by some historians as a “training exercise” or “target practice” before Allied invasions of islands closer to Japan, the bombing was so extensive that it created large bomb craters in the center of the island.
After the bombing, Satowan residents returned from Kutu and Moch to find their island transformed by Japanese military occupation and the subsequent American bombardment. In 1947, the Caroline Islands, now free from Japan’s occupation, became part of the US-governed Trust Territory of the Pacific. American foods, such as Spam, soon became a regular part of the Micronesian’s diet.
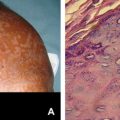
In the decades that followed, as they replanted taro fields, breadfruit trees, and coconut palms, the Satowanese began to observe an odd skin disease; they could neither attribute a cause to it nor find an effective treatment ( Fig. 1 ). Local health officials began to refer to it as “island psoriasis,” and residents began to refer to it as “spam,” after the processed food product that the skin lesions were said to resemble. Treatments included bleach, battery acid, cigarette burns, hot ashes, electrocautery, and surgical excision and were usually ineffective, resulting only in disease recurrence and disfigurement (Kino S. Ruben, Medical Officer, Chuuk Department of Health, personal communication, June 2007).

Investigation
In the summer of 2004, health officials from the FSM reported this epidemic on Satowan to the Tripler Army Medical Center on O’ahu hoping to find a definitive cause, an effective treatment, and a successful prevention strategy. Histopathologic specimens were obtained and reviewed, but no definitive diagnosis established. Two years later, the Polynesian Voyaging Society announced plans to sail traditional voyaging canoes from Hawai’i to Japan via Micronesia. In a partnership with Aloha Medical Mission (AMM), a series of medical clinics were organized in Micronesia to coincide with the arrival of the sailing canoes. Prior to departure, members of the AMM were contacted by the Hawai’i Department of Health and asked to further investigate this mysterious illness that had afflicted inhabitants of Satowan since World War II. While in Weno, Chuuk’s capital city, six affected Satowanese islanders were evaluated by members of the AMM, but tissue cultures were negative and histopathologic analysis was again inconclusive.
Around the same time, in the fall of 2006, a 29-year-old man from Satowan presented to an indigent care clinic in Portland, Oregon, with an 18-year history of enlarging verrucous plaques on his left lower extremity that started when he lived on Satowan ( Fig. 2 ). A tissue culture demonstrated M marinum . Consistent with previous reports from Chuuk health officials in 2004, he estimated that 10% of the people on his home island had similar lesions. In the summer of 2007, an outbreak investigation was initiated with local health aides on Satowan to determine the causative organism and potential risk factors for developing the condition. Thirty-nine cases of verrucous plaques greater than 3 cm in size and present for more than three months were identified, with the majority (74%) in males. The median age was 26.0 years, the mean duration of involvement was 12.5 years, and the longest period of involvement was 53 years. All but one case involved the upper or lower extremities, and the most frequently affected area was the knee (44%).

Related posts:
 Buruli Ulcer: Advances in Understanding Mycobacterium ulceransInfection
Buruli Ulcer: Advances in Understanding Mycobacterium ulceransInfection
 Dermatology Aboard the USNS COMFORT: Disaster Relief Operations in Haiti After the 2010 Earthquake
Dermatology Aboard the USNS COMFORT: Disaster Relief Operations in Haiti After the 2010 Earthquake
 Chagas Disease: Coming to a Place Near You
Dermatology in Botswana: The American Academy of Dermatology’s Resident International Grant
Chagas Disease: Coming to a Place Near You
Dermatology in Botswana: The American Academy of Dermatology’s Resident International Grant
 Widespread Use of Toxic Skin Lightening Compounds: Medical and Psychosocial Aspects
Human Immunodeficiency Virus and Leprosy: An Update
Widespread Use of Toxic Skin Lightening Compounds: Medical and Psychosocial Aspects
Human Immunodeficiency Virus and Leprosy: An Update
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


