Abstract
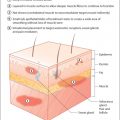
The appearance of the ageing face is a summation of foundation volume loss from recession of underlying skeletal support; skin volume loss from aging, ultraviolet damage and ‘rubbing’, and sagging of support muscles with gravity. Botulinum toxin is ideal for minimising muscle contraction but for full rejuvenation, it is best used in combination with solutions for other changed features. Upper lid bags if present must be corrected prior to attempting to eliminate forehead rhytids with botulinum toxin or the patient will look tired, lifeless, unnatural and often be unable to function well. Blepharoplasty (excision of skin and muscle) may be performed with correction of ptosis (levator repositioning) and often brow fixation (endoscopic brow lift, internal brow fixation). Lower lid bags should be corrected before botulinum toxin to crow’s feet or they will sag further. Scarless transconjunctival surgery is an option. Fillers are an important part of the botulinum toxin rejuvenation process. Autologous fat is excellent as a foundation for the face and may be fine-tuned with hyaluronic acid. Nanofat is particularly good for lower lids, as is lower lid fat transplant to the tear trough in certain patients. CO 2 laser resurfacing erases fine lines and stimulates repair of the collagen framework in the skin. PRP, Viora radiofrequency and dermaroller are also told for collagen stimulation.
Key words
Botox, Dysport, Azzalure, filler, Restylane, Perlane, blepharoplasty, brow lift, fat transplant, carbon dioxide/CO 2 laser resurfacing, scarless blepharoplasty.
Hyaluronic acid
Laser resurfacing
Upper and lower blepharoplasty
Combination treatments
Brow lift, neck lift, suborbicularis oculi fat lift
Fat transfer and nanofat injections
Collagen stimulating combination treatments
Dermaroller
Platelet rich plasma
Ultherapy ultrasound/radiofrequency
Skin protection and rejuvenation products
Introduction
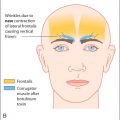
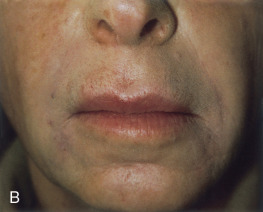
Botulinum toxin is good at preventing wrinkles in certain age groups. It is the ideal treatment for ‘wrinkles in motion’ (dynamic lines) and can even dissolve ‘wrinkles at rest’ (static lines) in patients with good skin tone (see Fig. 8.2 A and B). However, patients with poor skin tone, and deep crow’s feet at rest, will not get a good response from botulinum toxin alone ( Fig. 11.1 A and B). Those with furrowed brows but a low lash-brow distance, poor tone of their forehead skin and/or an excess of upper lid skin (dermatochalasis) will actually look worse if they lose further muscle tone after botulinum toxin. They need an alternative treatment.


Ageing skin sags for several reasons. The skin loses collagen, becoming thinner and less transparent as the parallel collagen fibres become cross-linked and misaligned. This is greatly accelerated by smoking and exposure to ultraviolet (UV) A and B rays. The time at which ageing starts is genetically predetermined: if a mother does not have a wrinkle until the age of 55, then her daughter with the same genes and habits may not either. Clearly, the extent to which the skin ages also depends upon environmental factors. If a mother has had an excessive exposure to the sun and smokes, when she does begin to age at 55, she will probably become severely wrinkled within a short time. On the other hand, if her daughter—with the same genes—avoids UV damage and smoking, she may well retain the tone in her skin for much longer.
It is sensible to educate all botulinum toxin patients on the subject of skin protection and recovery (‘stopping the clock’). Aesthetic nurse practitioners may spend time assessing the patients’ skin regime and, if necessary, tretinoin (the author campaigns against cancer-causing paraben preservative in creams, etc.), paraben free, can be prescribed.
Ageing of the face is also due to the recession of its skeletal support. The anteroposterior diameter of the skull lessens with time, and this encourages sagging in spite of an otherwise excellent skin tone. The diameter of the orbit increases from superomedially to inferolaterally, reducing support for the orbicularis oculi muscles and skin. Traditional cosmetic surgery replaces this lost support by excising skin and muscle (facelift, blepharoplasty). Facial implants, such as malar and chin implants, have been used. The author favours the natural reinforcement of the foundations of the face with autologous fat transplant, using nanofat for the periocular tissues. Laser resurfacing can tighten and ‘lift’ sagging structures. Brow lifts are being replaced by brow repositioning (internal brow fixation or an endoscopic brow lift), while blepharoplasties often include lateral canthal tendon plication to tighten the sagging areas over an expanded orbital rim.
The tone of the skin is actively enhanced with collagen-stimulating treatments such as dermarolling and serum plasma injections. Autologous fat brings stem cells and plasma factors with it, further nourishing and rejuvenating ageing skin. Hyaluronic acid fillers are used to finesse periocular volume replacement, as well as supplementing lost skeletal support with larger molecule fillers such as Perlane.
The ways in which patients should be selected for botulinum toxin are discussed in detail in earlier chapters. Some alternatives (see Table 11.1 ) are discussed here.
| Indication | Treatment |
|---|---|
| Crow’s feet at rest | Laser resurfacing, platelet rich plasma, radiofrequency Viora Reaction, hyaluronic acid skin boosters |
| Lower lid bags | Laser blepharoplasty, fat transplant, nanofat remodelling |
| Vertical frown with low lash brow distance | Endoscopic brow lift, hyaluronic acid |
| Frown with heavy upper lid skin | Upper lid blepharoplasties, brow repositioning, hyaluronic acid |
| Upper lip rhytids, mouth zone rhytids | Laser resurfacing, PRP, Dermaroller, radiofrequency Viora Reaction, hyaluronic acid |
| Platysma bands, neck rhytids | Lower facelift,Threads, Viora radiofrequency, PRP, skin boosters, Dermaroller. |
| Poor skin tone, sun damage | Restylane skin boosters, PRP, Viora radiofrequency, Dermaroller. Microdermabrasion, chemical peels, tretinoin, alphahydroxy acid skin regime, vitamins C and E serum, sun protection |
Hyaluronic acid and other fillers
‘Fillers’ are volume-replacing products that can be inserted with a cannula or injected into the skin. The principle behind their use is that, with age and sun damage, the face loses volume and so the skin sags.
Fillers are an essential part of a good cosmetic botulinum toxin practice.
Fillers are an essential part of a botulinum toxin practice. Like botulinum toxin, they are injectable and associated with almost no downtime. Unlike botulinum toxin, the most advanced fillers give an instant result. Within minutes, a patient can leave the office looking up to 10 years younger. Many of our patients routinely book in for a ‘top-up’ of their filler at the same time as their follow-up botulinum appointment, to maintain their rejuvenation as the clock moves forward. Current legislation in Ireland prohibits the injection of botulinum toxin by a nurse practitioner, unless specifically prescribed by a doctor. This is allowed in other countries such as the U.K., and this handbook is designed to enhance a nurse practitioner’s basic knowledge and safe practice with botulinum toxin. The same nurse practitioners are allowed to select and inject fillers and submucosal anaesthesia (but not nerve blocks). They are also experts in combination medical-grade collagen-stimulating treatments.
Hyaluronic acid
Hyaluronic acid occurs naturally in the body and is the main component of the vitreous gel of the eye. It was originally derived from cockerel combs but is now produced synthetically. Since the 1980s it has been used extensively in cataract surgery to prevent the cornea collapsing and to protect the corneal endothelium during surgery. It is now available in different consistencies for intraocular injection. Restylane was developed by an ophthalmologist in QMed for injection into the skin ( Fig. 11.2 ).
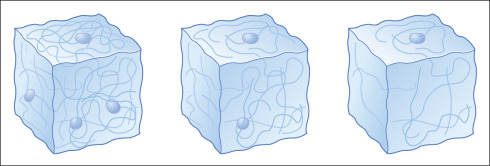
Hyaluronic acid is a pure substance, and the incidence of allergic reactions to it is very low. Patch testing is not required. Restylane and Perlane remain in the skin for nine months. Their molecules are gradually absorbed and replaced by water, which maintains the volume enhancement until the molecular framework collapses ( Fig. 11.3 ).
Many fillers are currently available on the market. Fat transplantation (the Sydney Coleman technique) offers a permanent solution, but is a semi-surgical procedure requiring time off work, and often more than one treatment session. At least 30% of the fat is absorbed, hence the need for a ‘top up’, but new microcentrifuged solutions of autologous fat (nanofat) are ideal for many oculo facial procedures, such as safe volume restoration at the superior and inferior orbital rims. A further benefit of autologous centrifuged fat is the accompanying platelet rich serum and its nutrients (the core part of a popular skin enhancing ‘vampire facial’).
In the past, routine cosmetic blepharoplasties included removal of all the orbital fat pads. The resulting gaunt look has long disappeared from fashion and volume is recognised as an essential part of youthful healthy skin. The author may sculpt fat in the lower lids, for example, but frequently transplants fat into the lacrimal fossae to restore rather than remove volume and minimise the dark circles under the eyes ( Fig. 11.4 A and B).


Hyaluronic acid is available in several ranges. The author continues to favour Perlane, Restylane and Restylane vital skin boosters by QMed. Skin boosters are popular for rejuvenation of face, neck, décolletage and hands, increasing hydration and elasticity for up to six months. Juvederm products appear to have a similar effect and the Belotero range of finer particled hyaluronic acid (Merz) is equally effective. Perlane, Restylane and Restylane fine line last for 9 months, but the author has evidence of Restylane fine line remaining in tear troughs for more than 24 months ( Fig. 11.5 ).

The author’s personal choice of product, based on experience, is currently as follows:
- ■
Perlane appears to be the most viscous, most enduring and the best for deep rhytids.
- ■
Restylane is of moderate viscosity, long lasting, good for deeper and superficial injections and the most versatile (d eep, superficial and lips).
- ■
Restylane fine line and Belotero Soft come with a 32-gauge needle and smoothly fill fine superficial rhytids, for example crow’s feet.
- ■
Restylane skin boosters and Belotero Soft are ideal for nourishing skin.
- ■
Sculptra (polylactic acid) is the synthetic filler of choice (if not using autologous fat) as a foundation in emaciated faces or faces with excessive lipoatrophy, for example after chemotherapy.
Indications
The choice of product depends on the area to be filled and on the volume required. Patients may also be restricted financially in their choice of treatment, which can be adapted to give the best value for their money. For example, Perlane may be best for deeper rhytids, but if a patient has both superficial and deep rhytids (e.g. a glabellar crease and nasolabial folds) and can only afford one syringe, 0.7 mL of Restylane may be used to treat both. Patients can be advised to plan for a full Perlane syringe in the future, and they should be made aware that the deepest rhytids compress the gel most quickly and require a top-up sooner. If there are no budgetary constraints, open as many syringes as are necessary to achieve the desired result ( Fig. 11.6 A and B). Failure to do so always leads to a dissatisfied patient.

It is important to analyse the facial features and then tell patients exactly what volume is required for an optimal result, for example 2× Perlane 0.7 for deep nasolabial folds; 1× Restylane classic 0.75 mL for lips; 1× Restylane fine line for cheeks. They will then appreciate that suboptimal results will be achieved with less and will not telephone the next day to say ‘the lines are still there’ if they buy only one syringe.
Patient preparation
Injections of hyaluronic acid without local anaesthesia are sore—the pain being a sensation of pressure rather than the possible ‘sting’ of botulinum toxin. Injections are usually superficial and so can be effectively anaesthetised topically with proprietary lidocaine/prilocaine cream (EMLA) or lidocaine 4% cream (LMX). Deeper injections, for example to the lips, can be very painful. It is recommended to choose either a filler containing local anaesthetic or to infiltrate local anaesthetic submucosally first.
Patients should be warned that preparation takes at least 30 minutes. They should arrive early, in order that the nurse can apply EMLA and cover (with Opsite or Clingfilm) the area to be treated. They can then relax before treatment. For the lips, tetracaine gel is applied to the gums after these have been dried with a swab. A dental syringe with a short 30-gauge needle is used to infiltrate Citanest (or lidocaine [lignocaine]) submucosally in the fornix. This works in 10 to 20 minutes. Sterex antiseptic cream is applied after the treatment and the patient is allowed to apply make-up.
Nasolabial folds
Some deep nasolabial folds are associated with a short upper lip and respond well to botulinum toxin treatment to the apex. Most deep folds, however, are best treated with volume replacement to the superolateral support structures of the face, replacing lost ‘suspension’ of the midface and therefore ‘lifting’ the nasolabial folds. Some patients require a surgical facelift, although it is not uncommon for a deepening of the nasal end of the fold to persist after an effective operation. Most patients presenting for botulinum toxin are not ready to consider major surgery at the time of their initial consultation and are thrilled to have a short-term ‘cheat’ with Perlane. Some will benefit from thread lifting, albeit for about 18 months before the threads dissolve.
Superficial filling can be very effective ( Fig. 11.7 A and B) and achieved either with Perlane or Restylane. Deep filling may take more than one session ( Fig. 11.8 A and B). Perlane may be placed in the superficial dermis of the nasolabial skin, deep to the epithelium. Deeper placement often fails to ‘lift’ the skin and may be ‘lost’ towards the sinuses. Warn the patient that this layer will become slightly compressed by facial movements and recommend a top-up over the same layer after 6 weeks. This compensates for the compression of the initial layer and achieves a long-lasting effect.