7
Other Papulosquamous Disorders
Parapsoriasis
• Two major forms of parapsoriasis are small plaque (lesions usually <5 cm in diameter) and large plaque (usually >5 cm); digitate dermatosis is a form of the former, whereas retiform parapsoriasis is a variant of the latter (Figs. 7.1 and 7.2).


Fig. 7.1 Small plaque parapsoriasis. A Small (<5 cm), pink slight scaly patches. B Digitate dermatosis with elongated finger-like lesions on the flank. Digitate dermatosis is the exception to the 5-cm rule as the lesions may measure 10 cm or more along their long axes. A, Courtesy, Gary Wood, MD, and George Reizner, MD.


Pityriasis Lichenoides et Varioliformis Acuta (PLEVA) and Pityriasis Lichenoides Chronica (PLC)
• In both forms, there are recurrent crops of papules with individual lesions spontaneously resolving over weeks (PLEVA) to months (PLC); only occasionally is there an obvious trigger (e.g. viral infection, medication); the entire course of the disorder can last for years.
• PLEVA occurs more commonly in younger age groups; it is characterized by widespread erythematous papules that are often crusted but may be vesicular or pustular (Fig. 7.3A–C).



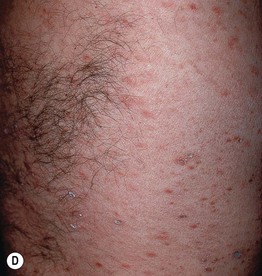

Fig. 7.3 Clinical spectrum of pityriasis lichenoides. In the acute form (PLEVA), widespread erythematous papules and papulovesicles are admixed with crusted lesions (A, B); sometimes there can be an ulcerative component (C). Lesions can heal with varioliform scars. Individuals with the chronic form (PLC) develop multiple red-brown papules, some of which have scale (D); these lesions often heal with hypopigmentation, especially in patients with darkly pigmented skin (E). A, Courtesy, Julie V. Schaffer, MD; B, Courtesy, Thomas Schwarz, MD.
•






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


