In order to address complex extremity injuries, the orthoplastic approach uses plastic, orthopedic, and microsurgical techniques and includes other disciplines to optimize limb salvage. This collaboration, if created early in treatment, allows for more expedient and individualized solutions to a variety of extremity injuries resulting in decreased hospital stay, fewer complications, and improved functional outcomes. The orthoplastic approach does not merely avoid amputation, but also improves patient function and quality of life in the short and long term.
Key points
- •
Complex extremity injuries should be treated with early multidisciplinary collaboration in an orthoplastic approach.
- •
Using a multidisciplinary orthoplastic approach can help avoid unnecessary extremity amputations.
- •
There may be improved functional outcomes when implementing a multidisciplinary orthoplastic approach.
Introduction
The orthoplastic approach to lower extremity reconstruction uses the strength of a multidisciplinary team and the synergy of principles and techniques from orthopedic and plastic surgeons. Although the orthopedic and plastic surgeons are the clinical leaders of the team, there are several critical members that support this approach, including vascular surgeons, infectious disease specialists, musculoskeletal radiologists, physical therapists, prosthetists, pain management physicians, and a specialized nursing staff. This collaboration leads to improved patient outcomes, optimized conditions for bone healing, expediting soft tissue coverage, decreasing length of hospital stay, and avoidance of complications and revision surgeries. The orthoplastic approach not only avoids amputation but also improves patient function and quality of life in the short and long term.
Indications and contraindications
With the advent of negative pressure wound therapy, the number of lower extremity trauma cases referred for soft tissue reconstruction has decreased, thus resulting in the referral of more complex cases to regional centers. Therefore, many of the patients who may be candidates for extremity salvage and orthoplastic techniques may be transferred from outside institutions, and therefore, it is critical to educate referring centers as to what are potential indications for referral. Open fractures in patients with comorbidities, Gustilo III injuries, dysvascular limbs, concomitant nerve injuries (especially lacking plantar sensation), foot/ankle soft tissue loss, compartment syndrome, crush or blast injuries, or patients with additional social or psychological needs should be considered for transfer and would potentially benefit from a multidisciplinary approach.
Preoperative evaluation and special considerations
Typically, the orthopedic surgeon stabilizes fractures, whereas the plastic surgeon provides soft tissue coverage. The orthoplastic approach can combine these strengths in a variety of operative circumstances. In the case of lower extremity trauma, the orthopedic surgeon may be providing the initial assessment of the wound as well and determining whether higher rungs of the reconstructive ladder will be necessary to obtain soft tissue coverage with reconstructive plastic surgery assistance. In the case of oncologic defects or diabetic limb salvage, the orthopedic and plastic surgeon can perform preoperative evaluation and planning, intraoperative decision making, and postoperative care in synchrony. Particularly in the trauma setting, the evaluation by both an orthopedic and a plastic surgeon may result in a different result than if only 1 specialist was making the decision between extremity salvage and amputation. This difference may be due to lack of familiarity with more complex reconstructive techniques or fixation options, misconceptions with concomitant nerve injury, differences in length of soft tissue and bony recovery, or complexity of socioeconomic variables. Especially in the latter circumstances, one can see why all members of the orthoplastic team are critical.
Surgical procedures
The orthoplastic approach has been well described, and therefore, in later discussion, the authors touch on the advancements in theory and techniques and discuss the burgeoning areas where rapid change will occur in the coming years.
Pediatric IIIC Injuries
Although Gustilo type IIIC injuries are not exceeding common, and those injuries in children are even less so (2.6% of all open pediatric tibial fractures), the stakes become high at an exponential rate when the case does present itself. Regional tertiary referral centers may be fortunate enough to have a team skilled in pediatric microsurgery dedicated to pediatric vascular injuries, but this is rare.
There are few data regarding Gustilo IIIC injuries in children. Traditionally, based on literature by Gustilo and colleagues and subsequent studies from the 1980s, Gustilo IIIC injuries were rarely considered for extremity salvage because of the high rate of eventual amputation. However, there have been advances since then in all aspects of lower extremity trauma care. We are more facile with microsurgical techniques and skeletal fixation as well as with trauma and critical care in general. Ricci and colleagues have demonstrated in the adult population that Gustilo IIIC injuries fare no worse than single-vessel Gustilo IIIB injuries with regard to salvage and complication rates and advocated that we are justified in pursuing extremity salvage. We will likely never have the data to demonstrate the same in the pediatric population, but should be compelled to pursue salvage considering the adult outcomes.
In a pediatric IIIC injury, special care must be given to bony healing and growth potential. If there is a significant bony defect, external circular frame fixation may be needed with acute limb shortening and sequential lengthening. A fresh vascular repair may delay the start of limb lengthening. Separately, limb lengthening or bony transport may be complicated by poor soft tissue coverage, which may ultimately necessitate a flap reconstruction in a patient with complex lower extremity vasculature. In these ways, a collaborative approach is critical.
Medial Femoral Condyle to Foot and Ankle
Both persistent nonunion and avascular necrosis (AVN) occur in the setting of vascular compromise. In foot and ankle surgery, the talus and navicular bones are prone to such pathologic condition because of their poor blood supply, which may be further compromised by trauma or surgical manipulation of the surrounding tissues. Long-standing AVN or nonunion may result in painful debilitating arthrosis of the tarsal, subtalar, or ankle joints. Arthrodesis may be the final reconstructive option for such situations. In patients with comorbidities, such as peripheral neuropathies, diabetes, nutritional deficiency, peripheral vascular disease, and tobacco use, the rate of failed primary fusion with nonunion is 28% to 48%.
Various revision options are available for failed foot and ankle fusion, and some include autogenous bone grafting as a way of restoring bone stock to the fusion site for structural support. When the use of conventional procedures, including the use of nonvascularized bone grafts, has failed, more advanced techniques are required, such as vascularized bone grafts.
The medial femoral condyle/trochlea is a versatile graft that can be used as vascularized cortical bone, cancellous bone, cartilage, periosteum, or a chimera of the above. The medial femoral condyle can include skin or muscle to augment the soft tissue with variable size that can help achieve the desired union. ,
Arteriovenous Loop Fibula
Ankle arthrodesis is a solution in select cases of severe pain resulting from ankle arthrosis or may be used as a salvage procedure after failed total ankle arthroplasty. The type of ankle arthrodesis is dictated by the degree of deformity, soft tissue status, and bone quality. In cases with minimal or no deformity, in situ arthrodesis may be performed with minimal arthrotomy or arthroscopically using a percutaneous fixation technique. More severe cases may require open realignment and internal fixation.
When a nonunion potential exists, the role of bone grafting comes in. Potential for union may be compromised by infection, bone defect, osteonecrosis of the talus, and previous nonunion. The source of bone graft is dictated by the amount and type required. The amount of bone graft needed depends on available bone stock, which may be compromised by previous surgery, trauma, or debridement in the setting of infection. The type of bone graft needed may be structural or nonstructural and conventional or vascularized. The distal fibula, distal tibia, and iliac crest are commonly used for nonvascularized bone grafts. The medial femoral condyle, iliac crest, and free fibula are commonly used sources for vascularized bone graft.
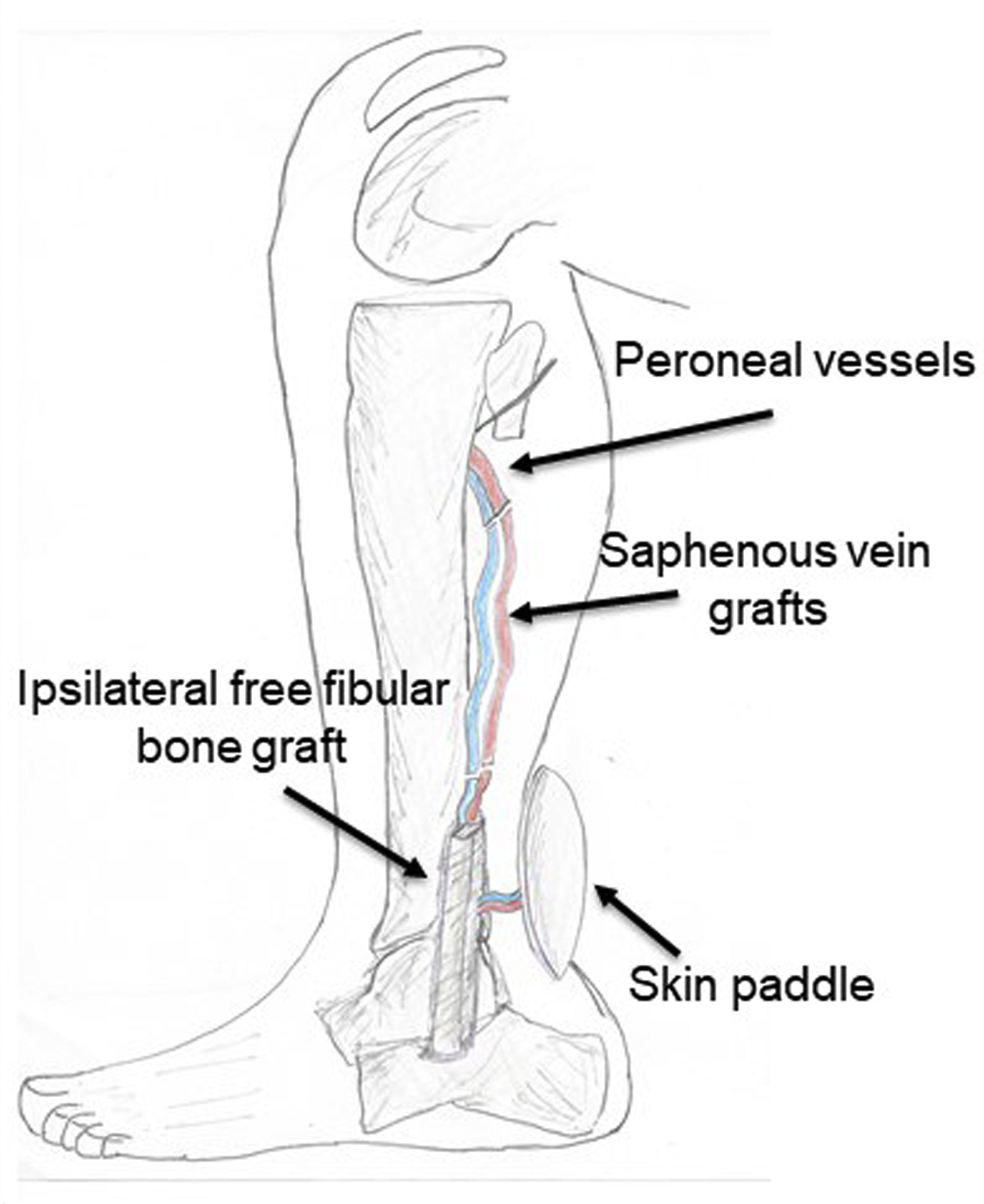
In cases whereby a significant bone defect is present, the use of vascularized fibula is most appropriate. In order to avoid contralateral morbidity and distal dissection for recipient vessels, the authors use an ipsilateral “AV loop” vascularized fibula. Surgical technique includes debridement of nonviable bone and soft tissue, ipsilateral free fibula harvest, and lengthening of the pedicle to the fibula. To lengthen the reach of fibula, saphenous vein grafts are anastomosed proximally to the native peroneal vessels, and then the artery and vein of the fibula pedicle are anastomosed to vein grafts ( Fig. 1 ).
Lymphatic Bypass
Consideration of persistent posttraumatic lymphedema has not been emphasized when it comes to extremity reconstruction. Although it is recognized that patients that experience significant lower extremity trauma develop some degree of lymphedema, the prevalence and severity are not well described; the cause and lymphatic anatomy have not been described until recently. It is now known that in the lower extremity, the lymphatic vessels originate on either side of the toes, on the foot, and at the lateral thigh. These lymphatics originate just deep to the dermis and travel in the subcutaneous tissue toward the popliteal, femoral, and superficial and deep inguinal nodal basins. In the upper extremity, the superficial lymphatics run with the main subcutaneous veins and do not appear to have major connections with the deep lymphatic system. Based on these anatomic studies, soft tissue injuries in these regions, especially degloving injuries or Morel-Lavallee lesions, may disrupt continuity of lymphatic channels and predispose patients to lymphedema. This finding would make sense in theory, but there are few to no supporting data.
Part of the reason that we have not paid enough attention to lymphedema in our population is because there were not good diagnostic tools or solutions for secondary lymphedema until recently. With the popularization of indocyanine green lymphangiography, the reason certain patients with extremity trauma and reconstruction develop lymphedema and others do not is slowly being elucidated. An interesting observation by Van Zanten and colleagues was that patients who underwent skin grafts, local flaps, or free muscle flaps for extremity reconstruction generally did not have restoration of lymphatic flow. In contrast, Slavin and colleagues found that patients who had fasciocutaneous or musculocutaneous free flaps for extremity reconstruction did have restoration of lymphatic flow. Therefore, the type of tissue transferred (and therefore the type of flap used) and whether it is rich in lymphatics may be critical. In addition, not just the type of flap, but also the orientation and inset of the flap at the extremity may be more important than initially thought because lymphatics have axiality and directionality. Just as inosculation of blood vessels exists, the same is thought to be true for lymphatics. Therefore, if a patient is seen with a circumferential defect of an extremity that was reconstructed with skin grafts and subsequently develops lymphedema, one might consider whether transfer of a free fasciocutaneous flap would provide a bridge of lymphatics to assist in proximal lymphatic transport. More anatomic studies need to be performed on deep lymphatics and the presence of lymphatics (or lack thereof) in muscles.
The development of lymphovenous bypass and vascularized lymph node transfers has given us yet another tool to potentially treat lymphedema. Lymphovenous bypass involves the anastomosis of lymphatics distal to the injury to veins in the area. This technique allows the excess lymphatic fluid at the distal aspect of the extremity to pass through the venous system to the proximal extremity, thereby bypassing the damaged and nonfunctional lymphatics in between. Lymphovenous bypass is not always an option, especially if there has been severe trauma to the area or long-standing lymphedema, which would result in potentially sclerosed and functionless lymphatics. Vascularized lymph node transfer is an alternative option that involves transfer of lymph nodes as a free flap to an area that is bereft of functional lymphatics. The transplanted lymph node is thought to act as a “sponge” for excess lymph. Although the mechanism is not completely clear, the transfer of functional lymph nodes is thought to cause sprouting of new lymphatics and induce new lymphatic collateral pathways via growth factor signaling. It will also allow for lymphaticovenous drainage, as lymph will flow into the node and can exit via venous outflow. These techniques have primarily been used in iatrogenic lymphatic injuries from oncologic extirpation but have much potential for any cause of secondary lymphedema.
Secondary Aesthetic Refinements
Although limb salvage is the primary goal, salvage rates are quoted at or greater than 90% in tertiary centers, and therefore, these once secondary aesthetic concerns are now considered much more important to the patient and the surgeon. A secondary surgery rate of near 30% for aesthetic reasons following lower extremity reconstruction using perforator flaps was reported by Hui-Chou and colleagues.
Multiple tools are at the disposal of the reconstructive surgeon to aid in the process: direct excision or debulking, tissue expansion, surgical and nonsurgical scar modification, laser treatment, and suction-assisted lipectomy, the latter of which is the most commonly performed technique. Lower extremity aesthetic considerations should not be of a secondary concern, but should be part of the ultimate reconstructive algorithm for lower extremity limb salvage.
Revisions or subsequent procedures
Some of the more common revisions necessary for patients who have undergone orthoplastic procedures include bone grafting of previous defects and soft tissue flap debulking. A common sequence of events for trauma patients includes (1) multiple debridements to create a healthy wound bed, (2) concurrent bony fixation with placement of an antibiotic spacer or beads as needed, (3) soft tissue coverage with locoregional or free flap, (4) removal of antibiotics spacer with bone grafting (Masquelet technique), and (5) soft tissue debulking as needed.
Bone grafting usually occurs several months after initial reconstruction and requires reelevation of the flap to gain access to the osseous defect. If a free flap was initially performed, care will need to be taken to protect the pedicle as the flap is reelevated. Even if the flap pedicle is injured during the reelevation, there should have been sufficient neovascularization from the periphery to supply the previously transferred tissue, but this is variable and flaps that have been in place for years can be compromised from pedicle injury.
Especially for reconstruction of the foot and ankle, long-term functionality may be compromised by a flap that is too bulky. It is a problem that requires patience on behalf of both the patient and the surgeon. Muscle flaps will undergo a significant amount of atrophy over time, and even fasciocutaneous flaps will decrease in size significantly as edema decreases over the course of months. Therefore, a flap that initially seems too bulky may end up having a near perfect contour. The authors usually assess this potential issue at a visit between 6 and 12 months, depending on the type of flap that was performed. Most often patients complain that they cannot fit into the appropriate footwear, or less often, that the bulk of the flap affects their gait. If the flap is on the plantar surface of the foot, it may prevent normal stance, or may even prevent clearance of the ground during the swing phase. Often these issues are not clear early on, as the patient is non-weight-bearing and is initially not wearing a normal shoe. If debulking is deemed necessary, it can be performed with direct excision or defatting of the undersurface of the flap, by liposuction of a fasciocutaneous flap, or with a combination of both. Again, the pedicle should be protected, especially when performing blind techniques like liposuction. If a perforator flap was performed, location of the perforators should be considered when planning direct excision.
Case demonstration
Case 1
Orthoplastic reconstruction of a Gustilo IIIC injury in a pediatric patient
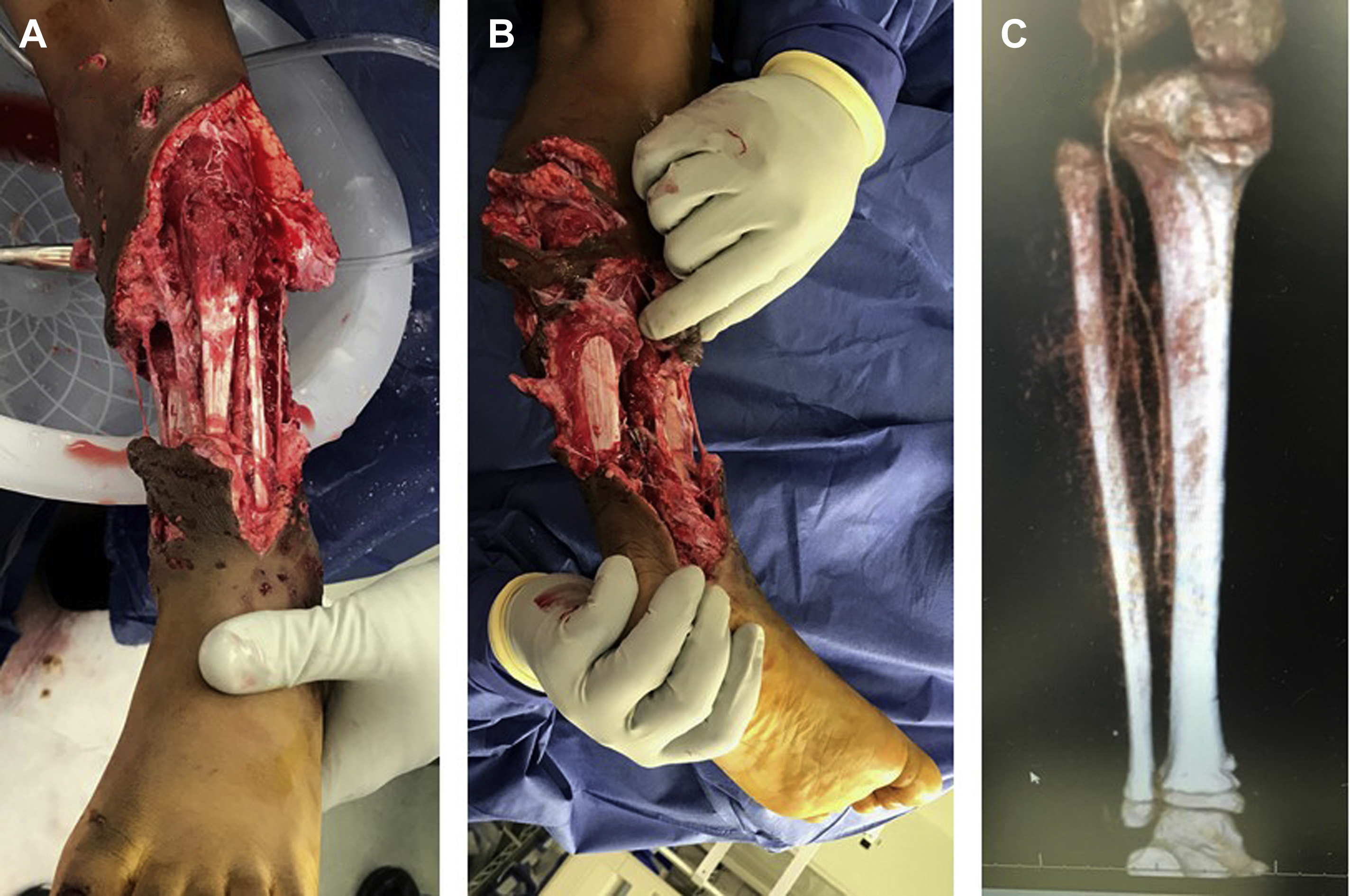
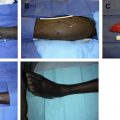
A 7-year-old boy was airlifted to our pediatric institution after an extensive pit bull dog-bite injury to his left lower extremity (LLE). The patient presented with a severely mangled extremity below the knee with bone exposure, but no fractures. Both dorsalis pedis and posterior tibial pulses were absent, and the foot was cold to touch with no sensation. On computed tomographic (CT) angiography, there was an abrupt cutoff of all 3 lower leg vessels at the level of the mid tibia ( Fig. 2 ). The patient was immediately taken to the operating room (OR) where he underwent extensive debridement and, by using his right great saphenous vein, arterial bypass was performed to both the anterior and the posterior tibial arteries to reestablish blood flow to the foot and leg ( Fig. 3 ). Three days later, the patient returned to the OR for soft tissue coverage using a free latissimus dorsi myocutaneous flap. The anastomosis was performed to the posterior tibial artery (above the bypass graft) using the junction of the subscapular and circumflex scapular arteries as a flow through arterial conduit ( Fig. 4 ). The patient eventually had successful skin grafting of the remainder of the flap ( Fig. 5 ). Two years after the injury, the patient’s leg remains viable with gross sensation intact and no limb length discrepancy.
Related posts:
 Propeller Flaps in Lower Extremity Reconstruction
Propeller Flaps in Lower Extremity Reconstruction
 The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
The Medial Sural Artery Perforator Flap in Lower Extremity Reconstruction
 Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
Free-Style Free Perforator Flaps in Lower Extremity Reconstruction
 Microsurgical Reconstruction of the Lower Extremity in the Elderly
Microsurgical Reconstruction of the Lower Extremity in the Elderly
 The Anterolateral Thigh Perforator Flap
The Anterolateral Thigh Perforator Flap
 Lower Extremity Reconstruction in the Pediatric Population
Lower Extremity Reconstruction in the Pediatric Population
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


