What is orthognathic surgery?
Orthognathic surgery is the surgical correction of abnormalities of the mandible, maxilla, or both. The underlying abnormality may be present at birth or may become evident as the patient grows and develops or may be the result of traumatic injuries. The severity of these deformities precludes adequate treatment through dental treatment alone.
 What are the main osteotomies performed in orthognathic surgery?
What are the main osteotomies performed in orthognathic surgery?
1. Maxilla:
a. Le Fort I osteotomy
i. One-piece
ii. Segmented
2. Mandible:
a. Sagittal split ramus osteotomy
b. Transoral vertical ramus osteotomy
c. Transcutaneous vertical ramus osteotomy
 What are the facial categorizations?
What are the facial categorizations?
Mesocephalic: equal vertical facial thirds
Brachycephalic: broader, shorter, square face
Dolichocephalic: ovoid and narrow face with an increased lower third
 What are the different classifications of skeletal relationships?
What are the different classifications of skeletal relationships?
See Figure 65-1.
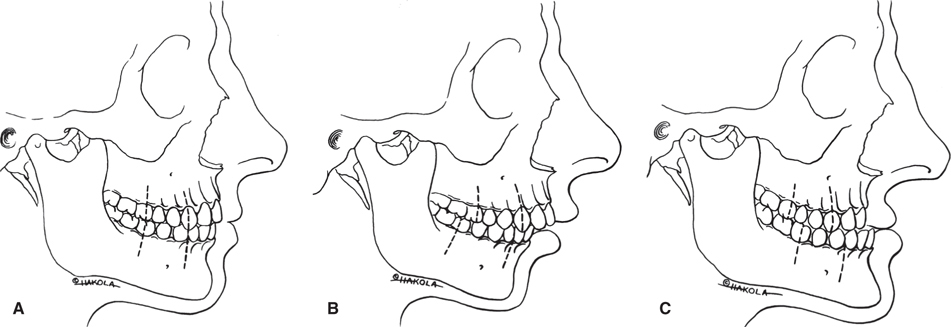
Figure 65-1 A: Class I orthognathic. B: Class II retrognathic. C: Class III prognathic. (Reproduced with permission from Ferraro JW. Fundamentals of Maxillofacial Surgery. New York, NY: Springer-Verlag Inc.; 1997.)
 How do you perform a dentofacial analysis?
How do you perform a dentofacial analysis?
A dentofacial analysis is a clinical examination of soft and hard tissue of the dentofacial complex assessing vertical and transverse proportions in a thorough, systematic, and consistent approach. Direct measurement of the patient’s resting and dynamic relationships is performed.
See Figure 65-2.
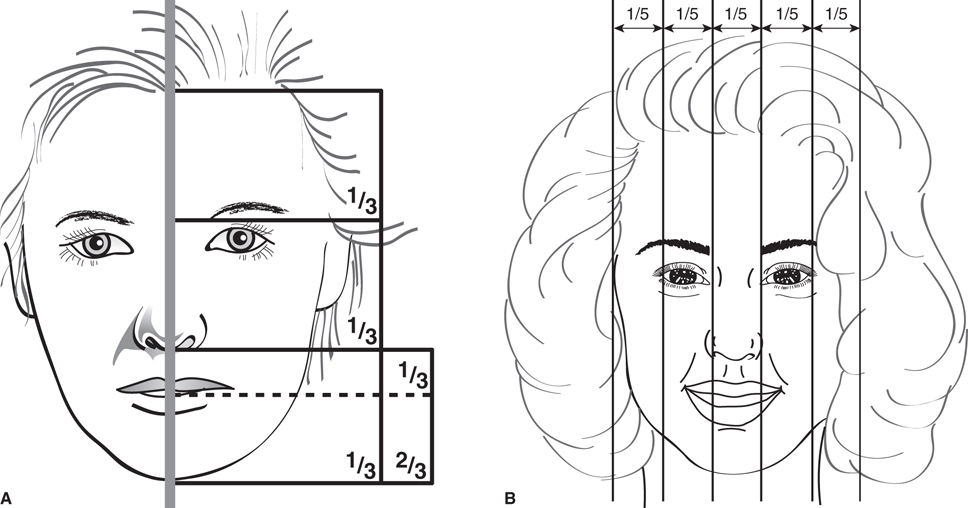
Figure 65-2 A: Reproduced with permission from Booth PW, Schendel SA, Hausamen JE. Maxillofacial Surgery. 2nd ed. Vol. 2. St Louis, MO: Churchill Livingstone; 2007. B: Reproduced with permission from Ferraro JW. Fundamentals of Maxillofacial Surgery. New York, NY: Springer-Verlag Inc.; 1997.
 What records are needed for treatment planning for orthognathic surgery?
What records are needed for treatment planning for orthognathic surgery?
1. Photographs:
a. Frontal view at rest
b. Frontal view with smile
c. Profile view at rest
d. Dental occlusal relationship
2. Plaster study models mounted on an articulator utilizing a face-bow transfer
3. Centric relation record
4. Cephalometric prediction
5. Radiographs:
a. Cephalometric radiographs
i. Lateral
ii. Posteroanterior
b. Panorex
 What are the most pertinent points/angles that should be traced on a lateral cephalometric radiograph?
What are the most pertinent points/angles that should be traced on a lateral cephalometric radiograph?
1. Sella (S): Center of the pituitary fossa of the sphenoid bone.
2. Nasion (N): Intersection of the internasal suture with the nasofrontal suture in the midsagittal plane.
3. Glabella (G): Most anterior portion of the frontal bone.
4. Orbitale (Or): Lowest point of the roof of orbit; most inferior point of the external border of the orbital cavity.
5. Subnasale (Sn): Point where the nose connects to the center of upper lip.
6. Anterior nasal spine (ANS): The tip of the ANS.
7. A-point: Deepest point of the curve of the maxilla between the ANS and the dental alveolus.
8. B-point: Most posterior point in the concavity along the anterior border of the symphysis.
9. Stomion superius: Most inferior point on the curve of the upper lip.
10. Stomion inferius: Most superior point on the curve of the lower lip.
11. Pogonion (Pg): Most anterior point on the midsagittal symphysis.
12. Gnathion (Gn): Midpoint between the most anterior and the inferior point on the bony chin.
13. Menton (Me): Most inferior point of the symphysis.
14. Porion (Po): Highest point of the ear canal; most superior point of the external auditory meatus.
15. Condylion (Co): Most posterior superior aspect of the condyle.
16. Gonion (Go): Most convex point along the inferior border of the ramus.
17. SNA:
a. Angle of sella, nasion, and A-point.
b. Relationship of maxilla to the cranial base—mean is 82 ± 2 degrees.
18. SNB:
a. Angle of sella, nasion, and B-point.
b. Relationship of the mandible to the cranial base—mean is 80 ± 2 degrees.
a. Angle of A-point, nasion, to B-point.
b. Relative position of maxilla/mandible to each other—mean is 2 ± 2 degrees.
c. N-ANS (mm) and ANS-Me (mm): Hard tissue proportion of the middle facial height to the lower facial height—mean ratio is 7:8.
20. MP-FH: Divergence of the mandible from the horizontal plane—mean is 25 degrees.
21. G-Sn-Pg′: Soft-tissue angle relative to facial form—mean is 12 ± 4 degrees.
22. G-Sn/Sn-Me: Soft-tissue proportion of the middle facial height to the lower facial height—mean ratio is 1:1 (Fig. 65-3).
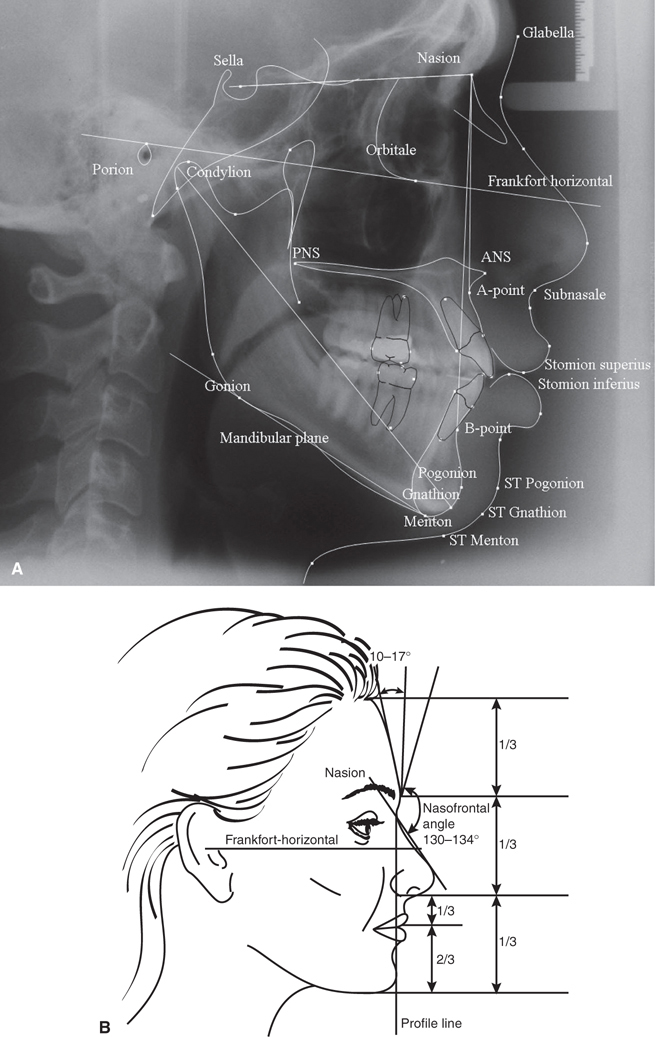
Figure 65-3 A: Lateral cephalometric radiograph. B: Profile of face demonstrating vertical and sagittal relationships. (B: Reproduced with permission from Ferraro JW. Fundamentals of Maxillofacial Surgery. New York, NY: Springer-Verlag Inc.; 1997.)
 What does a cephalometric prediction accomplish in treatment planning for orthognathic surgery?
What does a cephalometric prediction accomplish in treatment planning for orthognathic surgery?
A cephalometric prediction anticipates hard and soft-tissue changes of the planned surgery that cannot be visualized on the plaster model surgery. The purpose is to develop an accurate surgical treatment plan that will achieve the best functional and aesthetic results.
 What are the key features and surgical correction of short face syndrome?
What are the key features and surgical correction of short face syndrome?
The short face syndrome is characterized by a reduced facial height secondary to vertical maxillary deficiency
Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


