Oncoplastic Approach to Maximizing the Lumpectomy-Level II
Barry S. Rosen
Anne Peled-Warren
Toni Storm
Oncoplastic breast surgery involves applying plastic surgical principles to cancer operations to provide the best aesthetic outcome without compromising cancer treatment. The term “oncoplastic surgery” was first coined and popularized in the 1990s, with early papers describing a variety of different techniques to optimize reconstruction of lumpectomy defects (1,2,3,4,5). The central tenet of oncoplastic breast surgery is to “design the operation to fit the patient,” incorporating the patient’s desires and goals, their unique breast shape and size, and size and location of their breast cancer to find the perfect balance. Oncoplastic surgery is the ultimate example of personalized medicine, combining these variables so that “one size fits one.”
The challenge of breast-conserving surgery is to remove the tumor in its entirety without creating a deformity that would otherwise defeat the purpose of breast conservation (6,7,8). Oncoplastic breast surgery allows for the best of both worlds, optimizing both tumor excision and aesthetic outcome.
Oncoplastics is more of a philosophy than a technique, applicable to all patients undergoing breast cancer surgery. In the past, the goal was just to mitigate the deformity inherent with breast cancer surgery; now this has evolved to where we may offer to patients the option of possibly looking better after oncoplastic surgery than they did prior to their cancer diagnosis. A critical component of patient education is to explain that this is not about vanity, but rather recovery: living beyond a cancer diagnosis mandates removal of daily reminders of the trauma.
The defects created by tumor excision may be repaired by either displacing adjacent breast tissue to fill the space or replacing the tissue with an autologous flap. In the now-classic article published by Clough et al. in 2010 (9), oncoplastic surgery was divided into level I and level II techniques, based upon the amount of breast tissue removed and the need to perform a contralateral symmetrizing procedure. Most breast cancers can be managed by level I techniques, which entails hiding the scar and obliterating the defect after tumor excision. If cancer excision requires removal of 20% to 50% of the breast volume or if the patient desires a breast lift and/or reduction, level II techniques are ideal and are the focus of this chapter. Figure 10-1 presents an algorithm for considering oncoplastic options incorporating both clinical factors and patient preference.
Literature Review
Benefits of Oncoplastic Surgery
Given the excellent oncologic outcomes seen following lumpectomy and modern radiotherapy and systemic therapy protocols, with recent studies showing 5-year local recurrence rates of less than 5% (10), some surgeons may feel that lumpectomy alone is sufficient for many women with early-stage breast cancer, without adding the potential additional complexity of an oncoplastic procedure. Additionally, a lack of specialized training and concern about compromise in oncologic safety may be barriers to offering oncoplastic procedures (11,12). However, oncoplastic surgery has been demonstrated to improve outcomes and offers many benefits in addition to the expected improvements in aesthetic outcome and patient satisfaction.
Margins
Multiple studies have shown superior margin control during breast conservation when concurrent oncoplastic surgery is performed (13,14,15,16). Presumably, these improved rates stem from the ability of the oncoplastic surgeon to resect a larger volume of tissue when reconstruction of the defect will be included as part of the procedure. Additionally, many women undergoing oncoplastic reduction mammoplasty have symptomatic breast hypertrophy at baseline and would benefit from a significant reduction in breast volume, so a much larger volume of noncancerous breast tissue can be removed as part of the tumor specimen. This improvement in margin control
is seen in a meta-analysis by Losken et al. comparing outcomes from nearly 5,500 lumpectomy cases to 3,100 oncoplastic reduction mammoplasty cases (17). Overall tumor size was larger in the oncoplastic group (mean 2.5 cm compared to 1.2 cm), yet the positive margin rate was significantly lower in the oncoplastic group (12.4% vs. 20.6%, p < 0.0001). Another large single-institution study from MD Anderson Cancer Center including nearly 4,800 patients undergoing breast conservation echoed these findings, with a statistically significant reduction in positive margin rate when oncoplastic surgery was performed compared to lumpectomy alone (18).
is seen in a meta-analysis by Losken et al. comparing outcomes from nearly 5,500 lumpectomy cases to 3,100 oncoplastic reduction mammoplasty cases (17). Overall tumor size was larger in the oncoplastic group (mean 2.5 cm compared to 1.2 cm), yet the positive margin rate was significantly lower in the oncoplastic group (12.4% vs. 20.6%, p < 0.0001). Another large single-institution study from MD Anderson Cancer Center including nearly 4,800 patients undergoing breast conservation echoed these findings, with a statistically significant reduction in positive margin rate when oncoplastic surgery was performed compared to lumpectomy alone (18).
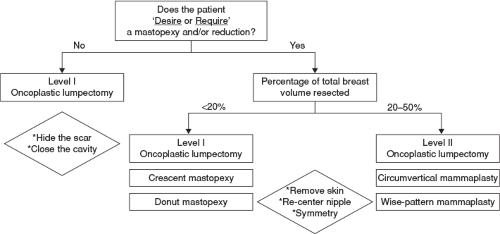 FIGURE 10-1 Algorithm for oncoplastic surgery options. |
Aesthetics/Patient-Reported Outcomes
Poor scarring and soft tissue defects left by lumpectomy alone can significantly impact the aesthetic outcome for women undergoing breast-conservation therapy (19,20,21). With oncoplastic procedures, particularly level II procedures, aesthetic outcome is significantly improved compared to lumpectomy alone, and may actually be improved from the patient’s preoperative baseline, with associated improvement in quality-of-life parameters (22,23,24). Additionally, for women who are candidates for either oncoplastic surgery or mastectomy and reconstruction, oncoplastic procedures have been shown to have significantly higher rates of patient-reported satisfaction with breast appearance and psychosexual outcomes (25,26).
Safety
Although oncoplastic surgery has many documented benefits, there are still some concerns regarding the long-term oncologic safety and the potential for increased surgical complications and possible associated treatment delay. While extended long-term data is still being gathered, shorter-term oncologic outcomes and immediate surgical outcomes are very favorable and comparable to lumpectomy alone.
First, looking at oncologic control, oncoplastic procedures have not been shown to negatively impact local–regional recurrence rates. A matched cohort study of nearly 1,400 patients with median follow-up of 7.2 years (27) showed equivalent 10-year local recurrence rates following oncoplastic procedures compared to lumpectomy alone. Other studies of patients undergoing oncoplastic surgery documenting longer-term follow-up demonstrate local regional recurrence rates similar to those historically seen with lumpectomy alone (28,29).
While margin positivity is lower following oncoplastic breast surgery, the consequence of a positive margin is higher, with meta-analyses showing mastectomy rates of 6.5% compared to 3.8% following traditional lumpectomy (17). Factors that may contribute to positive margins include variables intrinsic to the cancer such as high-grade cancers, lobular cancers, extensive ductal carcinoma in situ (DCIS), and HER-2/neu-amplified tumors (30,31,32).
A consensus conference was held in 2015 sponsored by the American Society of Breast Surgeons addressing factors that may reduce positive margin rates following breast conservation, summarized as the CALLER Toolbox (33). Updated recommendations and other prospective studies have discussed a number of extrinsic factors that may reduce positive margin rates including use of neoadjuvant chemotherapy, preoperative imaging beyond 2D mammography, surgeon use of ultrasound, intraoperative margin analysis, oncoplastic surgery, and routine cavity side-wall shaves (34,35,36). However, even if margins are positive after oncoplastic surgery, with proper tumor-bed marking, reexcision lumpectomy +/− repeat mammoplasty can be safely performed with low subsequent local recurrence rates (37).
Oncoplastic surgery has also been shown to be safe from a complications’ standpoint. Large meta-analyses comparing oncoplastic surgery to lumpectomy alone have shown equivalent rates of overall complications, in the range of 15% to 20% (17). Systematic review of oncoplastic surgery procedures shows the most common immediate surgical complications, including wound dehiscence, infection, and fat necrosis, occur in less than 5% of cases (14). Additionally, oncoplastic procedures have not been shown to lead to delays in adjuvant treatment (38). A recent population-based cohort study of over 1,700 patients demonstrated no time difference from surgery to chemotherapy whether the patient underwent lumpectomy, mastectomy, or oncoplastic breast surgery (39).
Related posts:
 Patient Selection for Breast-Conservation Therapy
Patient Selection for Breast-Conservation Therapy
 The Surgical Management of Locally Advanced and Stage IV Breast Cancer
The Surgical Management of Locally Advanced and Stage IV Breast Cancer
 Alternative Methods for Axillary Sentinel Lymph Node Dissection
Alternative Methods for Axillary Sentinel Lymph Node Dissection
 Optimizing Mastectomy Flaps Based on Breast Anatomy
Optimizing Mastectomy Flaps Based on Breast Anatomy
 Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
Liposuction as a Viable Treatment for End-Stage Upper Extremity Lymphedema
 Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Oncoplastic Techniques in Breast Conservation Therapy—The Plastic Surgeon’s Perspective
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


