Omental Flap for Pelvic Floor Reconstruction
Carrie K. Chu
Charles E. Butler
DEFINITION
Pelvic floor defects may result from colorectal, urologic, and/or gynecologic extirpation (ie, abdominoperineal resection, pelvic exenteration) for oncologic, infectious, inflammatory, or traumatic indications.
Goals of pelvic floor reconstruction include obliteration of dead space, prevention of pelvic and perineal hernia, avoidance of deep surgical site infection and pelvic sepsis, improved perineal wound healing, replacement of compromised perineal skin if necessary, and vaginal reconstruction when indicated.
ANATOMY
The male pelvis is typically narrower throughout, from the pelvic brim through the outlet. The cavity is overall shaped like an inverted cone, in contrast to the wider female pelvis that more resembles a short, wide cylinder.
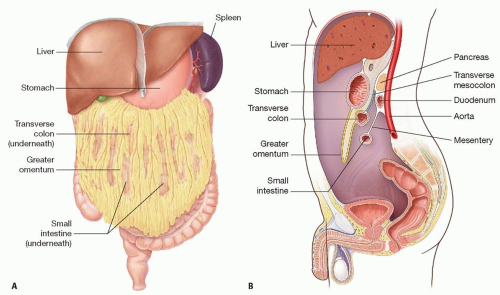
FIG 1 • A,B. The greater omentum extends from the greater curvature of the stomach and drapes over the large and small intestines while folding under itself toward the posterior abdominal wall. The posterior aspect of the reflection apposes the mesentery of the transverse colon.
The greater omentum, also called the gastrocolic omentum, is a curtain of adipose and lymphatic-rich tissue that extends from the greater curvature of the stomach and drapes over the large and small intestines while folding under itself toward the posterior abdominal wall. The posterior aspect of the reflection apposes the mesentery of the transverse colon (FIG 1).
The vascular supply of the omentum derives from the right and left gastroepiploic arteries. The right gastroepiploic artery is a terminal branch of the gastroduodenal artery, which comes off of the common hepatic artery originating from the celiac axis. The left gastroepiploic artery is a branch of the splenic artery.
Along the greater curvature of the stomach, gastric branches arise from both the right and left gastroepiploic arteries onto the anterior gastric wall, and the two vessels communicate in this manner. Multiple branches of these vessels supply the greater omentum (FIG 2).
The flap may be based on either the right or left gastroepiploic artery. The pedicle should be selected based on the likelihood of maximal flap length to reach the pelvis following full mobilization. The right-sided vessel is often positioned more favorably for pelvic coverage.
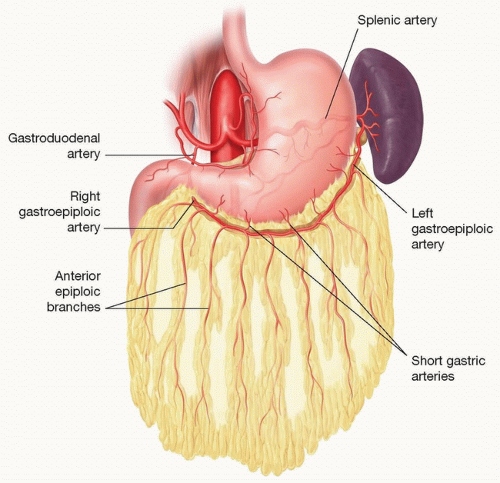 FIG 2 • The vascular anatomy and basis for the pedicled omental flap. |
PATHOGENESIS
Following removal of the rectum, the resultant void in the presacral space and pelvic outlet leaves noncollapsible dead space for fluid accumulation with infectious potential as well as a route for visceral herniation into the perineum. The volume of space is increased with additional resection of the bladder, prostate, uterus, and/or vagina.
Secondary defects of the pelvic floor may occur from traumatic, obstetric, or iatrogenic etiologies.
PATIENT HISTORY AND PHYSICAL FINDINGS
Special consideration should be given to the primary disease process and previous abdominal surgical surgery. Dense abdominal adhesions may render this flap unusable. Inflammatory processes or infectious complications may lead to distortion of the omental anatomy. Gynecologic oncologic surgeries often involve partial or total omentectomies. Prior procedures that may have compromised the source vessels of the right and left gastroepiploic vessels, including hepatectomy, pancreaticoduodenectomy, gastrectomy, and splenectomy, should all be noted.
Physical examination should focus on body habitus, abdominal torso length, abdominal surgical scars, hernias, and evidence of intra-abdominal obesity.
Pelvic radiotherapy may severely compromise the quality of the perineal skin.
IMAGING
No routine imaging is necessary for preoperative planning for omental flap harvest. Computed tomography is of limited utility in assessing omental bulk, though well-timed contrast studies may facilitate visualization of branches of the celiac artery, superior mesenteric artery, and proximal gastroepiploic arteries. Magnetic resonance imaging may provide better depiction of omental volume.
However, abdominal and pelvic cross-sectional imaging is often available as part of the primary disease workup. Review can yield useful information regarding dimensions of the pelvic inlet and outlet as well as the shape and depth of the presacrococcygeal space.
SURGICAL MANAGEMENT
Omental flaps are most useful for filling of dead space in the pelvic cavity and separation of the intra-abdominal contents from the perineum. When perineal skin replacement is necessary due to disease involvement or radiation injury, omental flap alone will likely not suffice. Consideration should be given to use of a myocutaneous or fasciocutaneous flap instead of or in conjunction with the omental flap, depending on the size of the pelvic cavity.
The omentum is also suitable for reconstruction of partial vaginectomy defects and can be used in conjunction with skin grafting for this purpose.4
Pelvic floor reconstruction using pedicled omental flaps generally takes place at the time of the primary extirpative procedure. The usefulness of omental flap for secondary pelvic reconstruction in cases of delayed wound healing, pelvic abscess, or wound dehiscence can be limited.
There is great individual variability in the bulk and dimensions of the greater omentum. Based on the characteristics of the omentum and the defect anatomy, each patient will require intraoperative evaluation and judgment regarding the appropriateness of this flap for pelvic reconstruction. The omentum may be used in combination with other myocutaneous flaps to accomplish the aforementioned goals.5
Preoperative Planning
No routine preoperative imaging is indicated, but the aforementioned elements in the history and physical should be noted in preparation for surgery.
Patients should be consented for thigh, gluteal, and abdominal wall donor-site alternatives, as the suitability of the flap is usually unable to be determined until the abdomen is opened.
Positioning
There are no specific positioning requirements beyond the conventional lithotomy or, less frequently, supine positions used during primary resection, though consideration should be given to prepping of alternative sites in case of inadequate omental mass or reach.
Approach
A major advantage of this flap is its intra-abdominal location. Exposure beyond the extent performed by the primary surgeon is usually unnecessary. Superior extension of an infraumbilical laparotomy incision is sometimes required.
In the setting of increasingly common laparoscopic or robotic procedures, the omentum can be similarly harvested using minimally invasive approaches with or without the assistance of a hand-assisted port for retraction.
TECHNIQUES
▪ Omental Flap Harvest With Right Gastroepiploic Pedicle
Omental flaps for pelvic reconstruction are most commonly performed at the time of primary operation. Upon laparotomy, the integrity, mass, and length of the omentum are assessed for suitability for pelvic reconstruction.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree