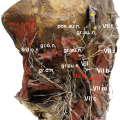
Intraorbital course of the frontal nerve (nf) and its branches exit from the orbit. so supraorbital nerve, str supratrochlear, red arrow fascial bands
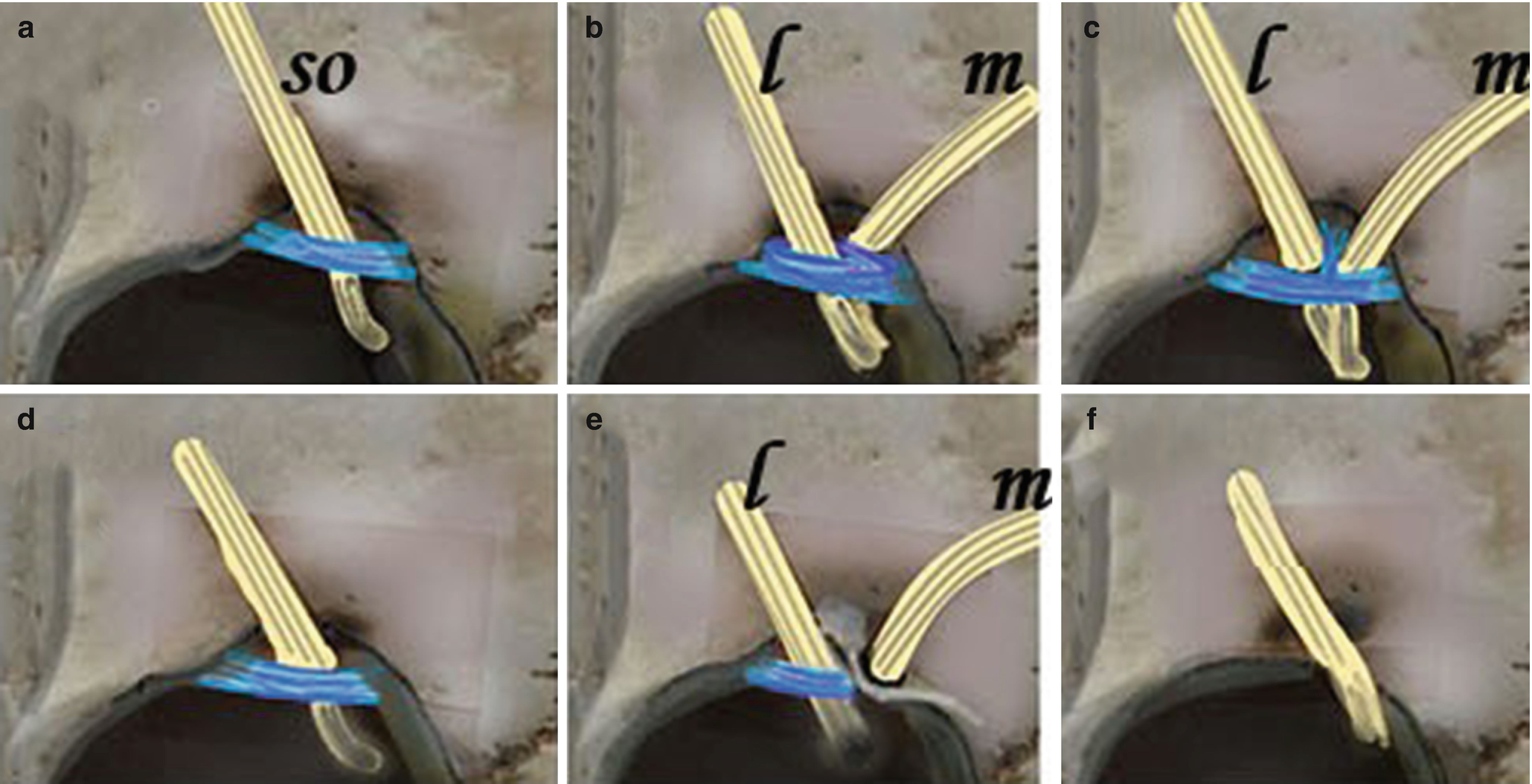
Different types of coverings of the supraorbital notch. (a) Fascial: single band spanning the notch. (b) Double fascial: parallel bands. (c) Inverted T: covering band plus a strand dividing the contents of the notch. (d) Fascial-osseous: consisting of fascial and bony parts. (e) Double passage: foramen and notch with covering band. (f) No opening: nerve and vessels passing over the rim
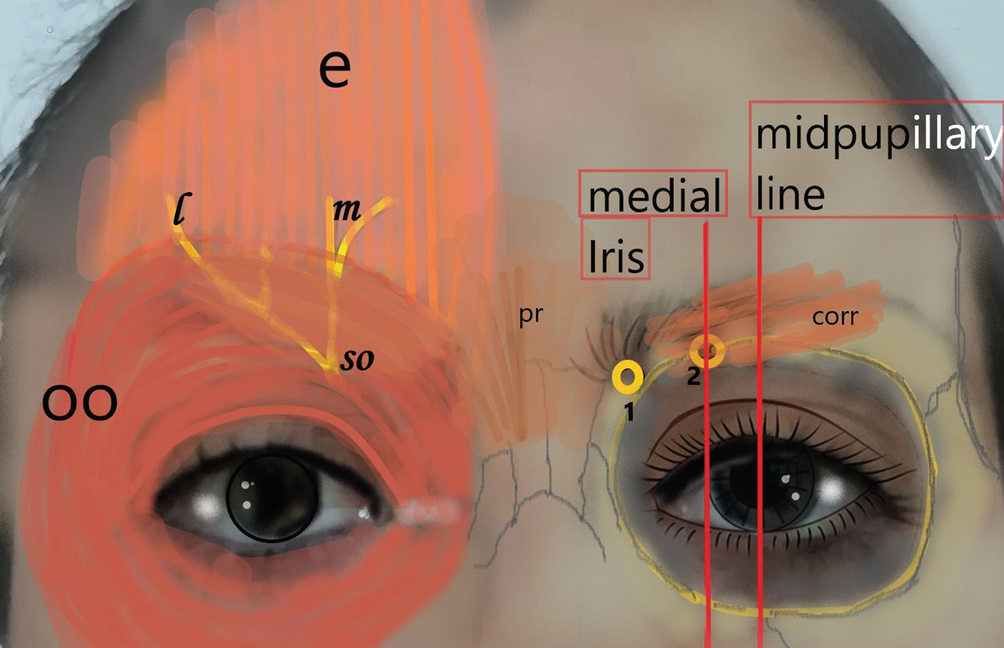
Localization of the passage points of the supratrochlear (1) and supraorbital (2) nerves at the forehead area. oo orbicularis oculi muscle, pr procerus muscle, corr corrugator supercilii muscle, so supraorbital nerve, m medial branch, l lateral branch of supraorbital nerve
There is a multitude of studies available on the proportion of notches versus foramen at the supraorbital rim. The prevalence of the SoN going through a bony foramen ranges from 26 to 50%, whereas a notch is present in 50–86% of reported specimens [13, 14]. A double passageway is found in up to 7% [29]. In 6%, yet another variant is one large notch through which both the SoN and StN passed [26]. Lastly, the SoN can go across the bony edge without any opening on the supraorbital margin. This type is called “pithecoid” meaning ape-like. In addition, all the above-described options can be different from side to side. Previous studies demonstrated that fascial bands covered the supraorbital notches in 83% of cases with simple bands being the most common followed by a partial bony covering [20] (Fig. 4.2). The StN passes the orbital rim through a notch in the majority of cases [13, 14, 26]. In 72% of these cases, the notch is covered by a band. In 8%, the nerve pierced through this band instead of running behind it. The prevalence of a true bony foramen as the passageway for the StN seems less clear. It is reported to range from 18 to 40% [26, 29].
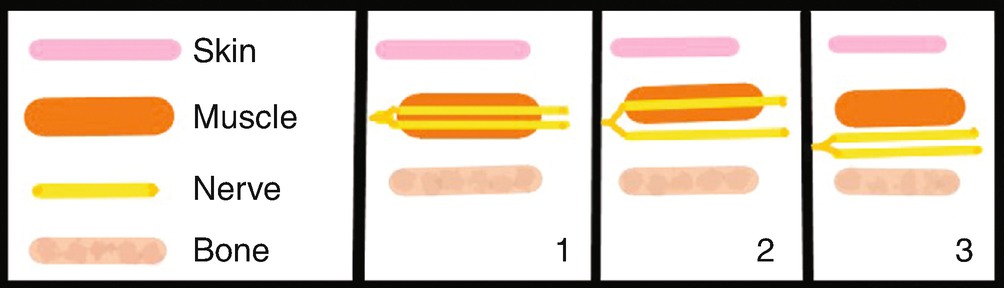
Patterns of the supraorbital nerve in relation to the corrugator muscle. The superficial/medial and the deep/lateral branches pass through the corrugator in (1). The medial one courses through and the lateral nerve continues underneath the muscle (2). Both branch of the nerve run underneath the muscle (3)
Patients who achieve only partial or no improvement of their migraine headaches after the paralysis of the corrugator through botulinum toxin, despite clearly pointing out the eyebrow and forehead area to be relevant pain localization, should be investigated for nerve compression at the supraorbital rim [4, 12, 27]. A possible stepwise method would be chemodenervation followed by injection of local anesthesia at the nerve passage at the rim with a delay of several weeks. In case of a significant change of symptoms following the second step, the anatomical characteristics could be elucidated.
4.2 Supraorbital Nerve
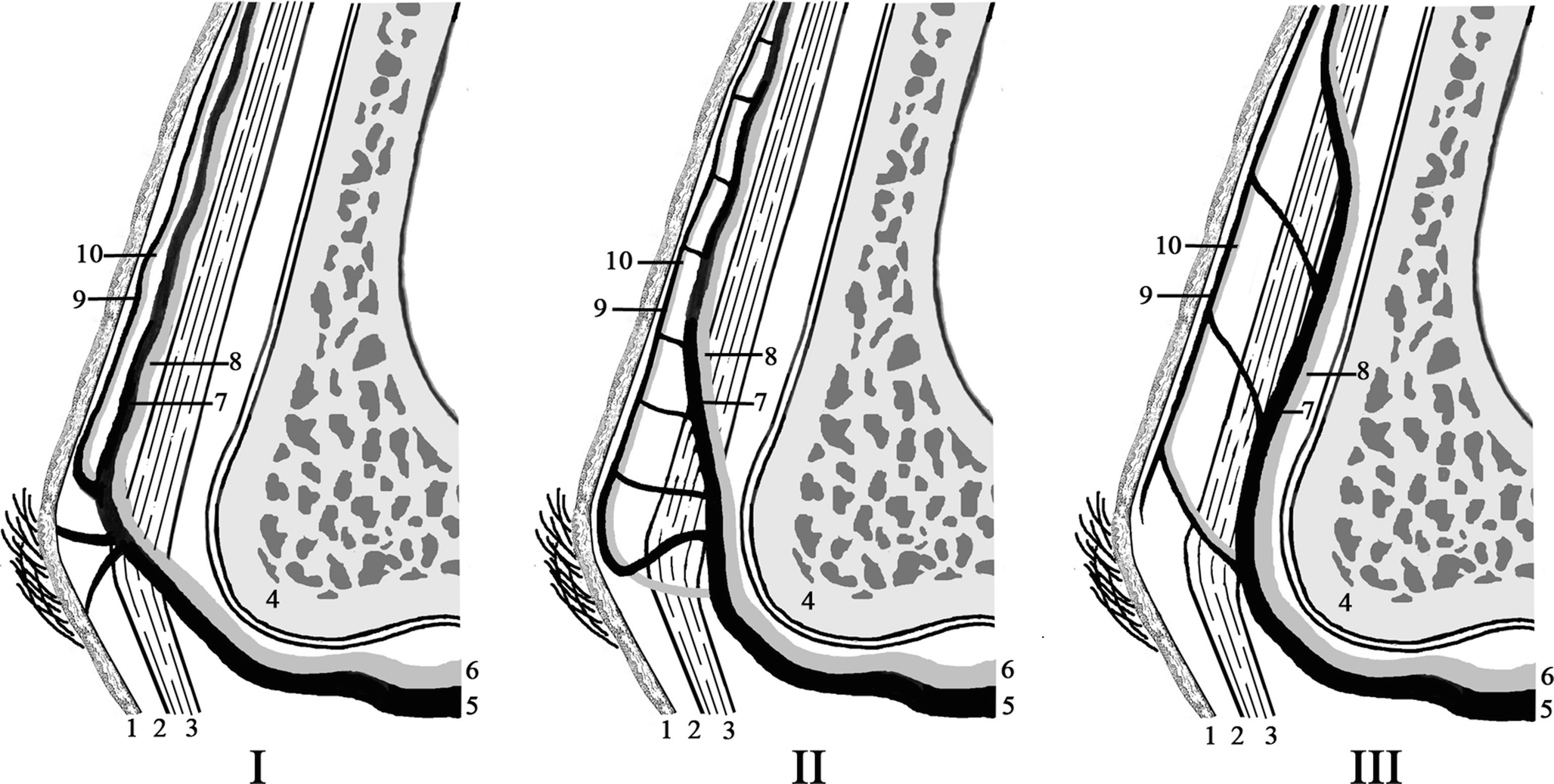
Schematic illustration of sagittal view of the neuroarterial structures in the forehead demonstrating to penetrate from subcutaneous (I-II) to submuscular (III) layer in three patterns: (1) the skin, (2) subcutaneous tissue, (3) frontalis muscle, (4) skull, (5) supraorbital artery, (6) supraorbital nerve, (7) deep branch of the supraorbital artery, (8) deep/lateral branch of the supraorbital nerve, (9) superficial branch of the supraorbital artery, (10) superficial/medial branch of the supraorbital nerve
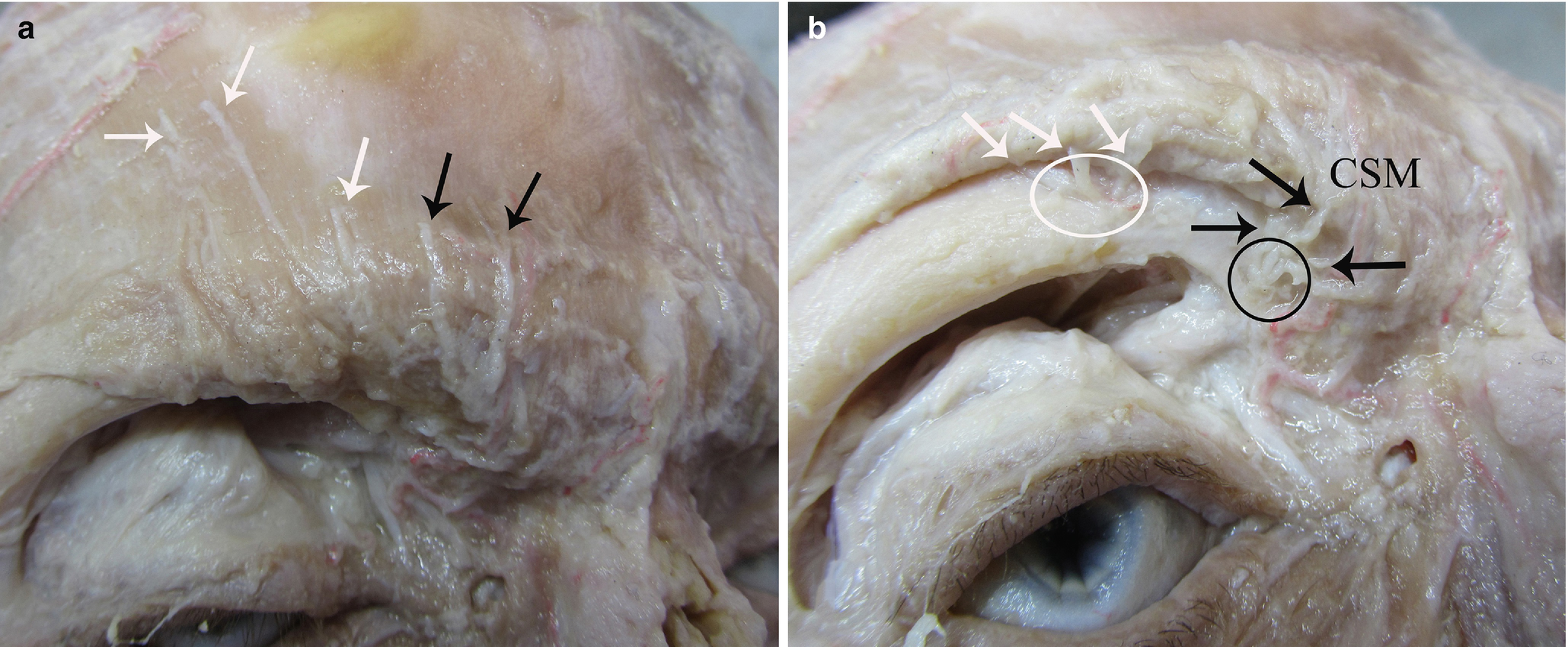
(a) Superficial and (b) deep dissection of the supraorbital region. The nerves of supraorbital (white arrow) and supratrochlear (black arrow) regions with compression points of supraorbital nerve (white ring) and supratrochlear nerve (black ring); nerves entrance points of the corrugator supercilii muscle (CSM)
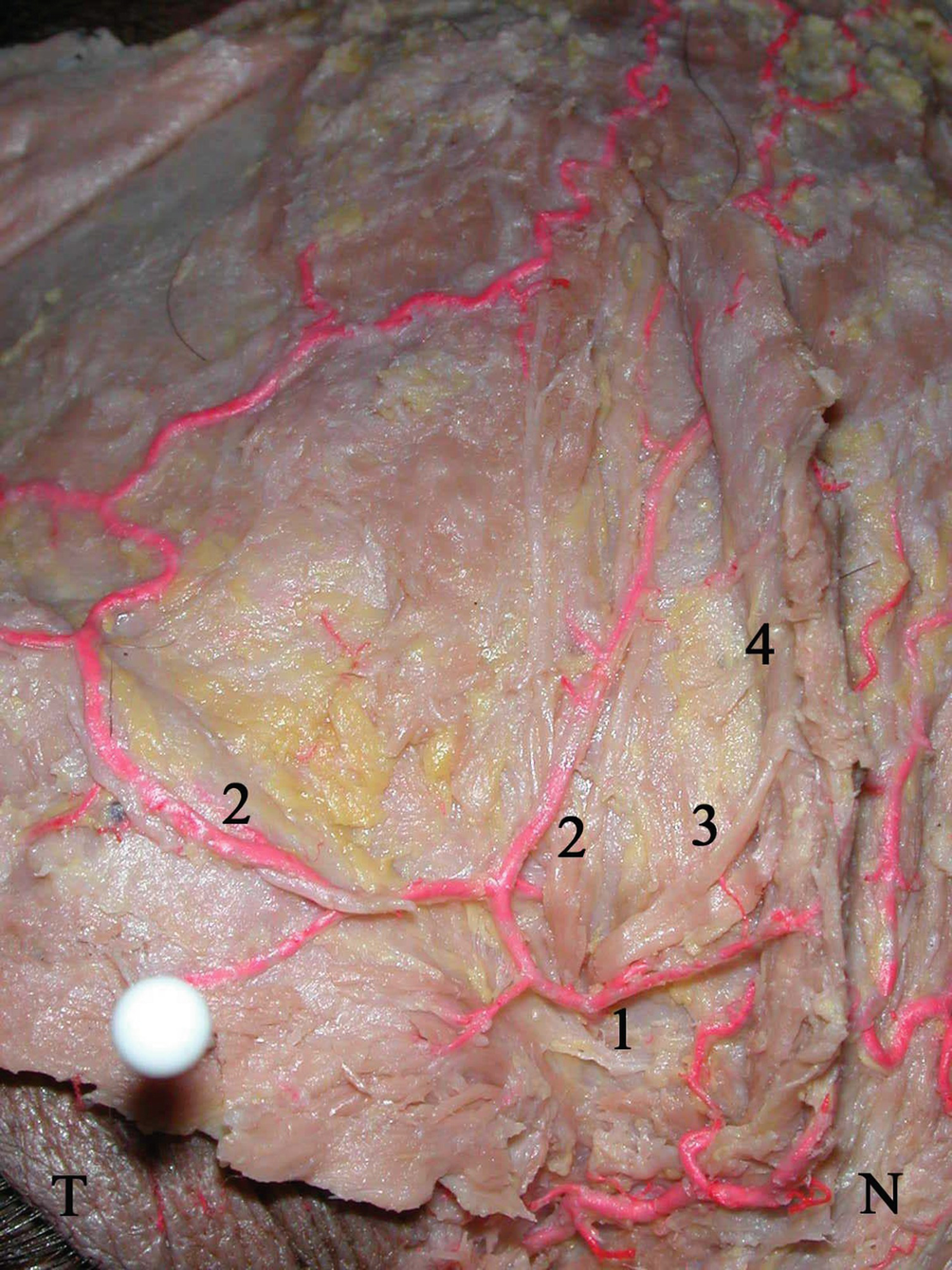
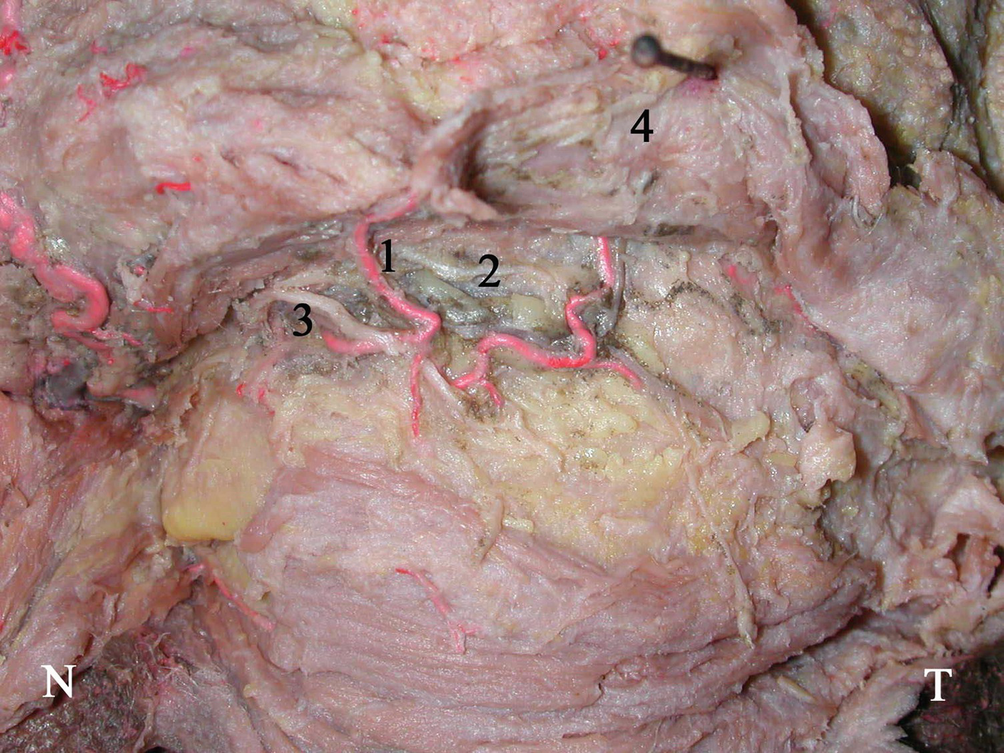
The supraorbital artery and the supraorbital nerve penetrating the frontalis muscle: (1) supraorbital artery; (2) superficial branch of supraorbital artery; (3) medial branch of supraorbital nerve; (4) frontalis muscle. N nasal side, T temporal side
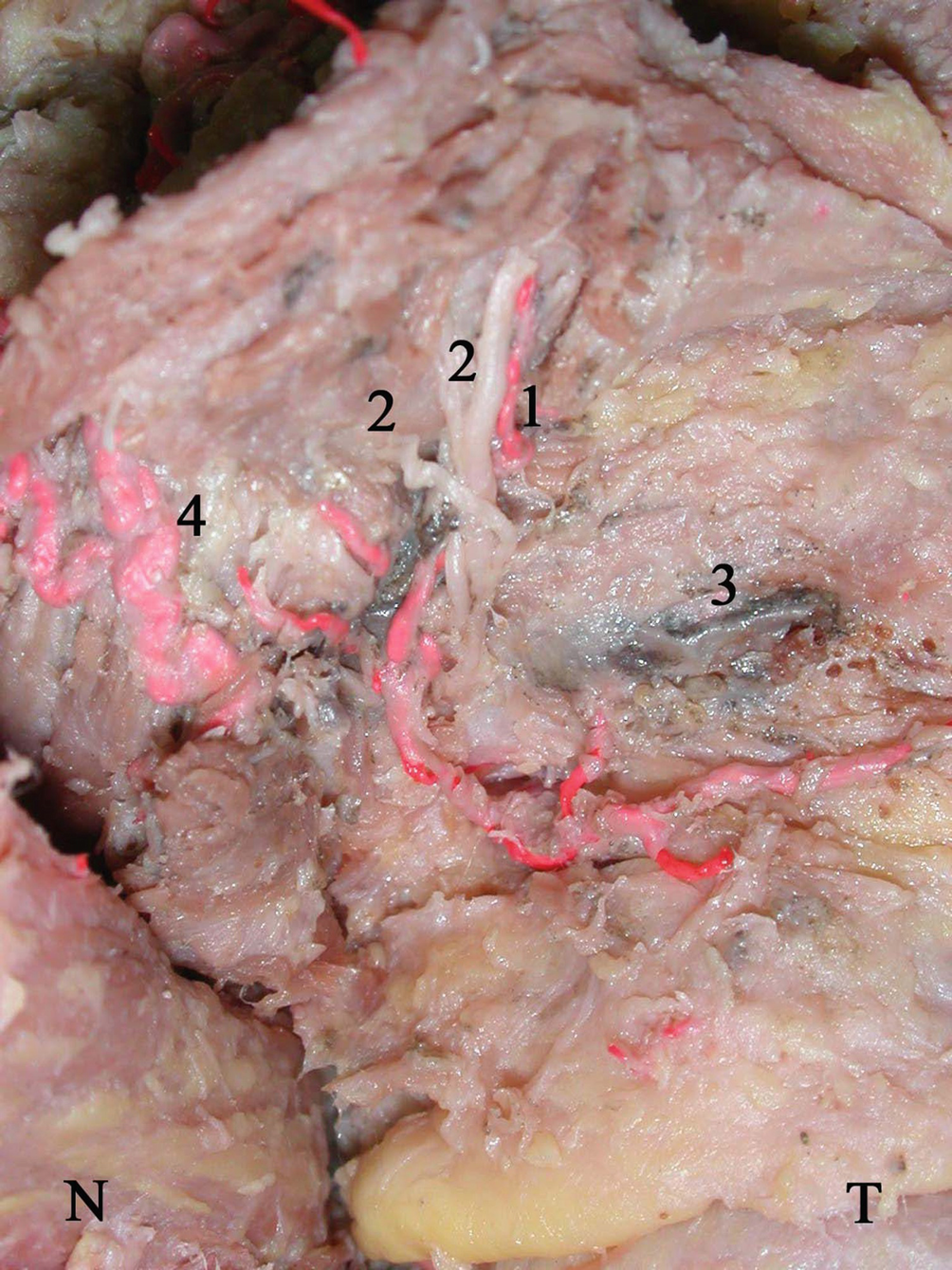
The deep/lateral branch of the supraorbital nerve exited the bone as two branches, usually one large and one much smaller: (1) deep branch of the supraorbital artery; (2) lateral branch of the supraorbital nerve; (3) supraorbital vein; (4) superficial branch of the supraorbital artery. N nasal side, T temporal side
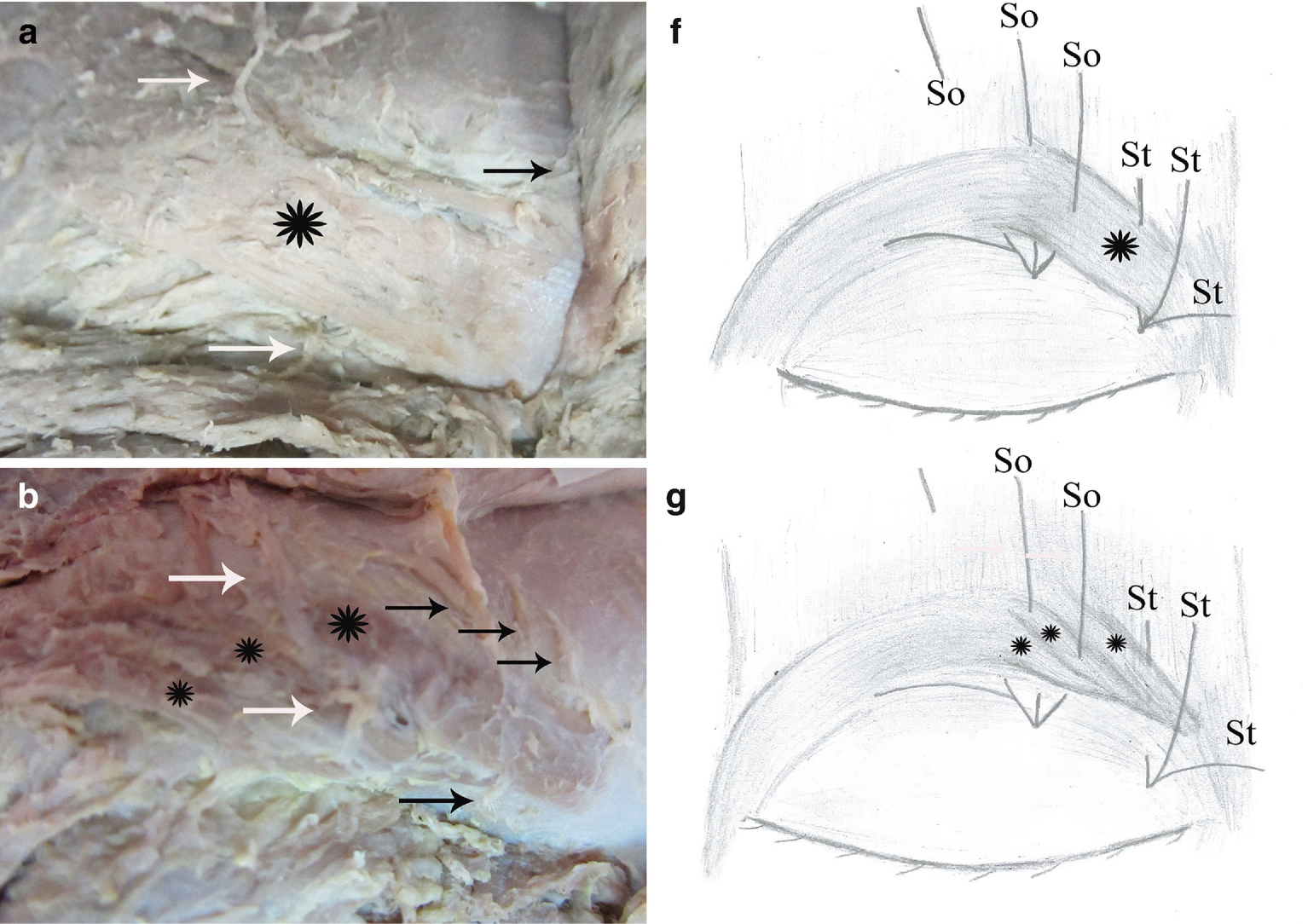
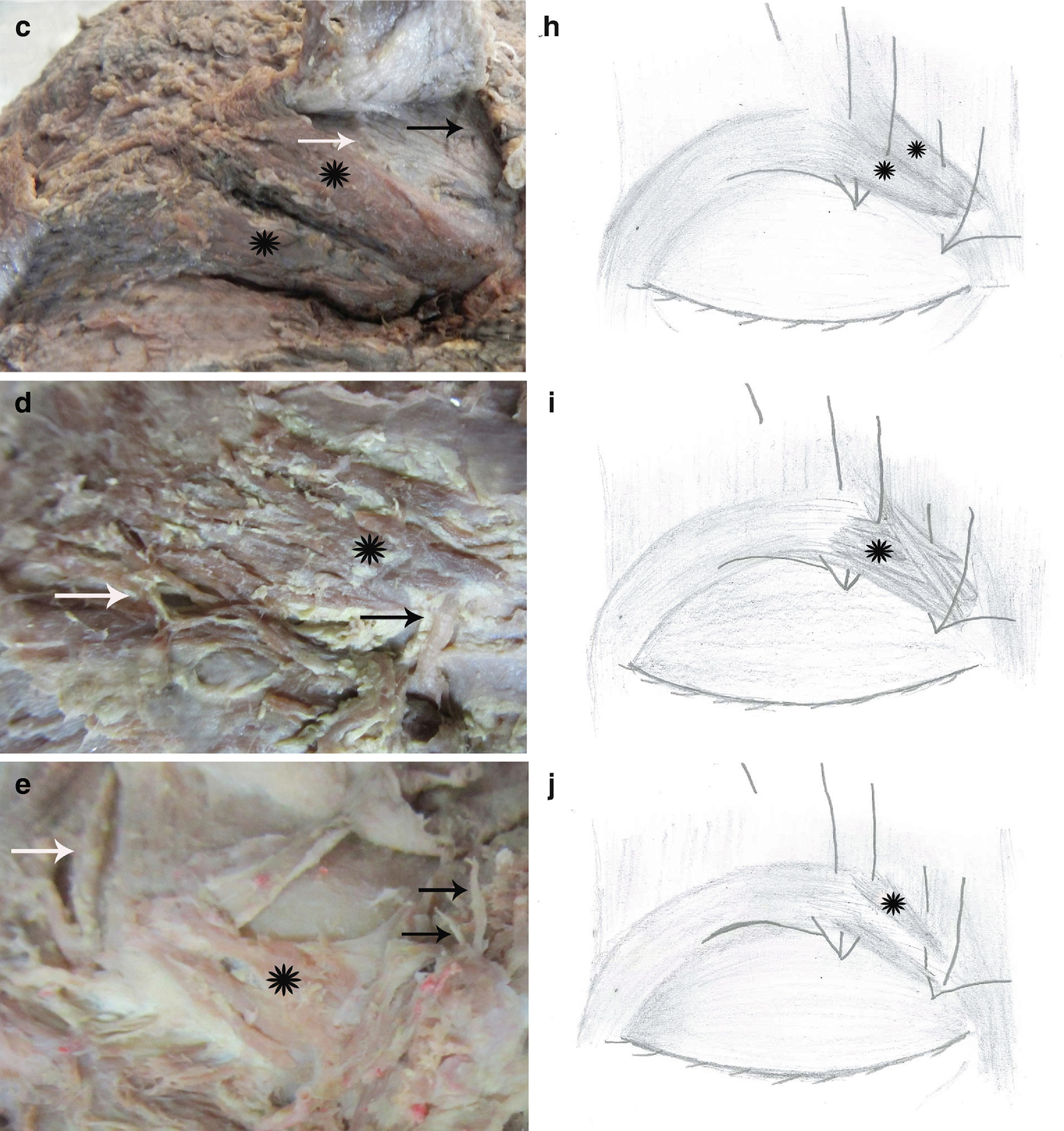
Five types of the corrugator supercilii muscle. (a, f) Rectangular type; (b, g) three bellied type; (c, h) dublicated type; (d, i) irregular muscle type; (e, j) hypoplasic type muscles. Black arrow and St: supratrochlear nerve; white arrow and So: supraorbital nerve; star: corrugator supercilii muscle
The corrugator muscle is lifted up with the supraorbital nerve passing through it. Photograph showing the deep/lateral branch of the supraorbital nerve and deep branch of the supraorbital artery in elevated frontalis muscle: (1) deep branch of the supraorbital artery; (2) supraorbital vein; (3) lateral branch of the supraorbital nerve; (4) frontalis muscle. N nasal side, T temporal side

The lateral branch of the supraorbital nerve arose from the bone and immediately subdivided into multiple small branches: (1) deep branch of the supraorbital artery; (2) lateral branch of the supraorbital nerve; (3) frontalis muscle; (4) supraorbital vein; (5) superficial branch of the supraorbital artery; (6) anastomosis with deep and superficial branches of the supraorbital artery. N nasal side, T temporal side
4.2.1 Points of Compression and External Landmarks
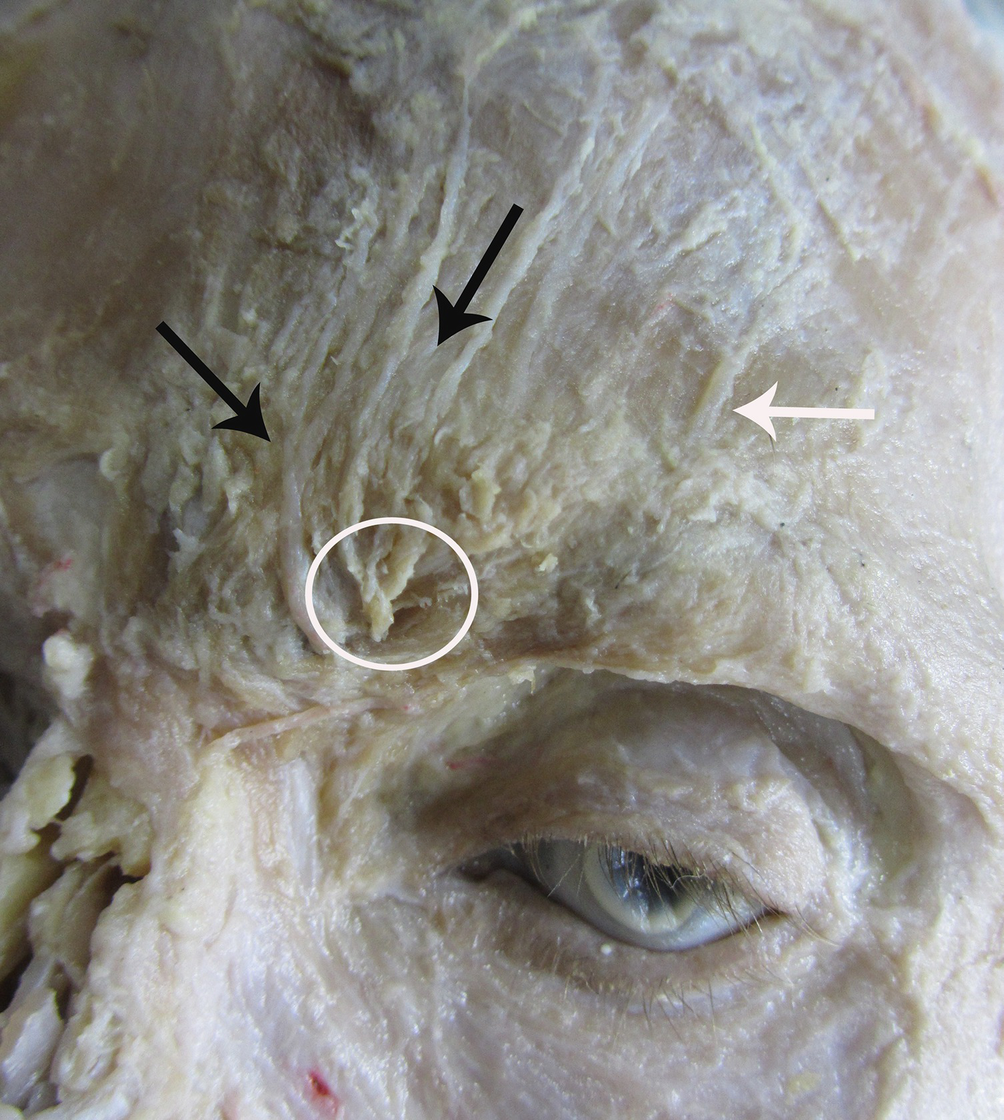
The supratrochlear nerve (black arrow) and supraorbital nerve (white arrow) are exited the superior rim of the orbit, frequently passing through their notches. Compression point of the supratrochlear nerves are implicited with fibrous bands (hole)
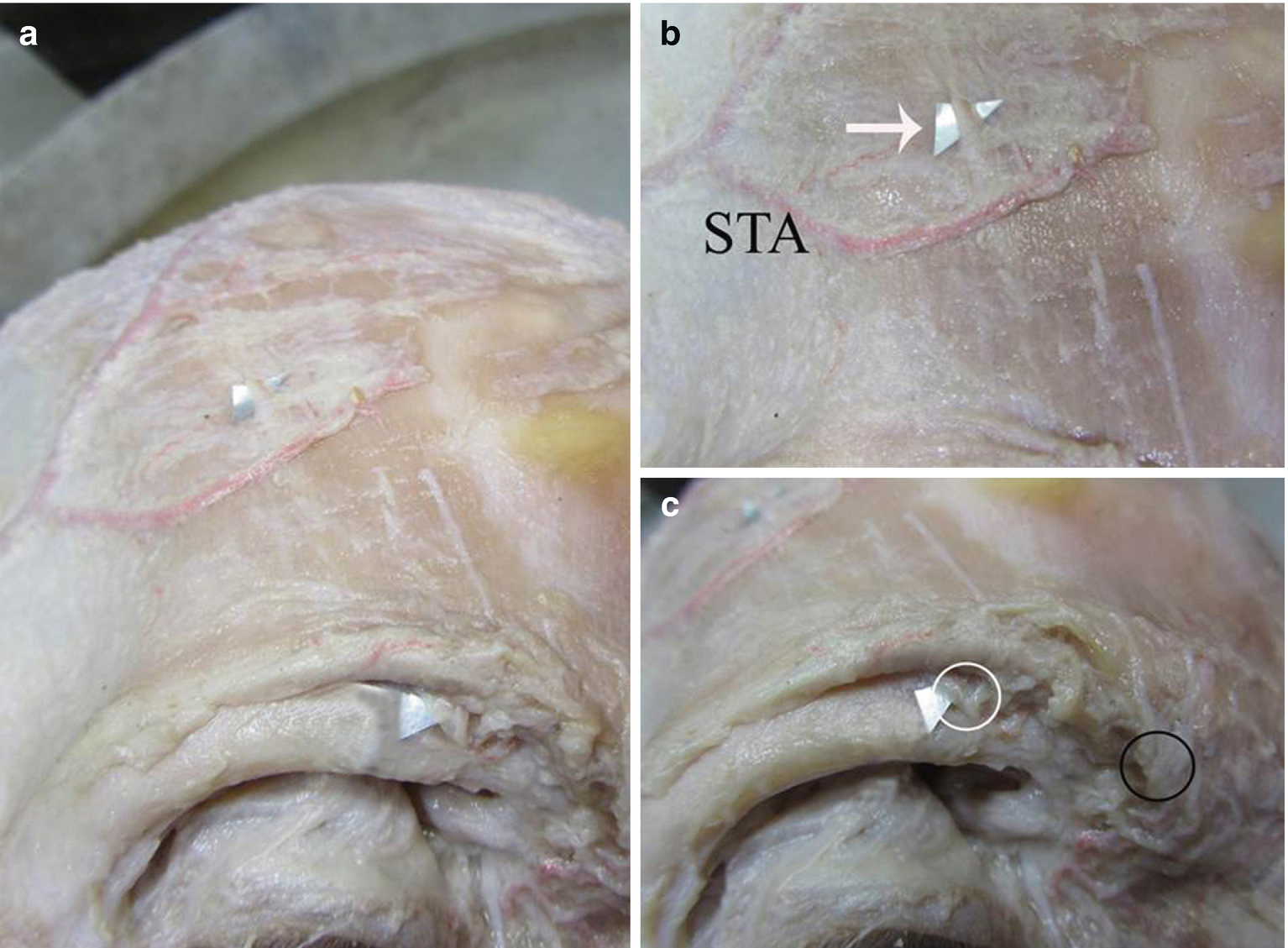
Demonstating of sensory innervation and blood supply with regional dissection (a) supraorbital, (b) forehead, (c) orbital. Compression points of supraorbital nerve (white ring) and supratrochlear nerve (black ring); nerves entrance points of the corrugator supercilii muscle. STA superficial temporal artery, white arrow: supraorbital nerve
Related posts:
 Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
 Anatomy of Craniofacial Nerves Regarding Migraine Surgery
Anatomy of Craniofacial Nerves Regarding Migraine Surgery
 Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
 Anatomy of the Vascularization and Innervation of the Human Scalp
Anatomy of the Vascularization and Innervation of the Human Scalp
 of Temporal Trigger Sites
of Temporal Trigger Sites
 of Occipital Trigger Sites
of Occipital Trigger Sites
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


