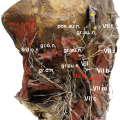
Convergence of frontal and occipital afferents. TG trigeminal ganglion, TNC trigeminal nucleus caudalis (Published with kind permission of © medsteps)
5.2 Anatomy
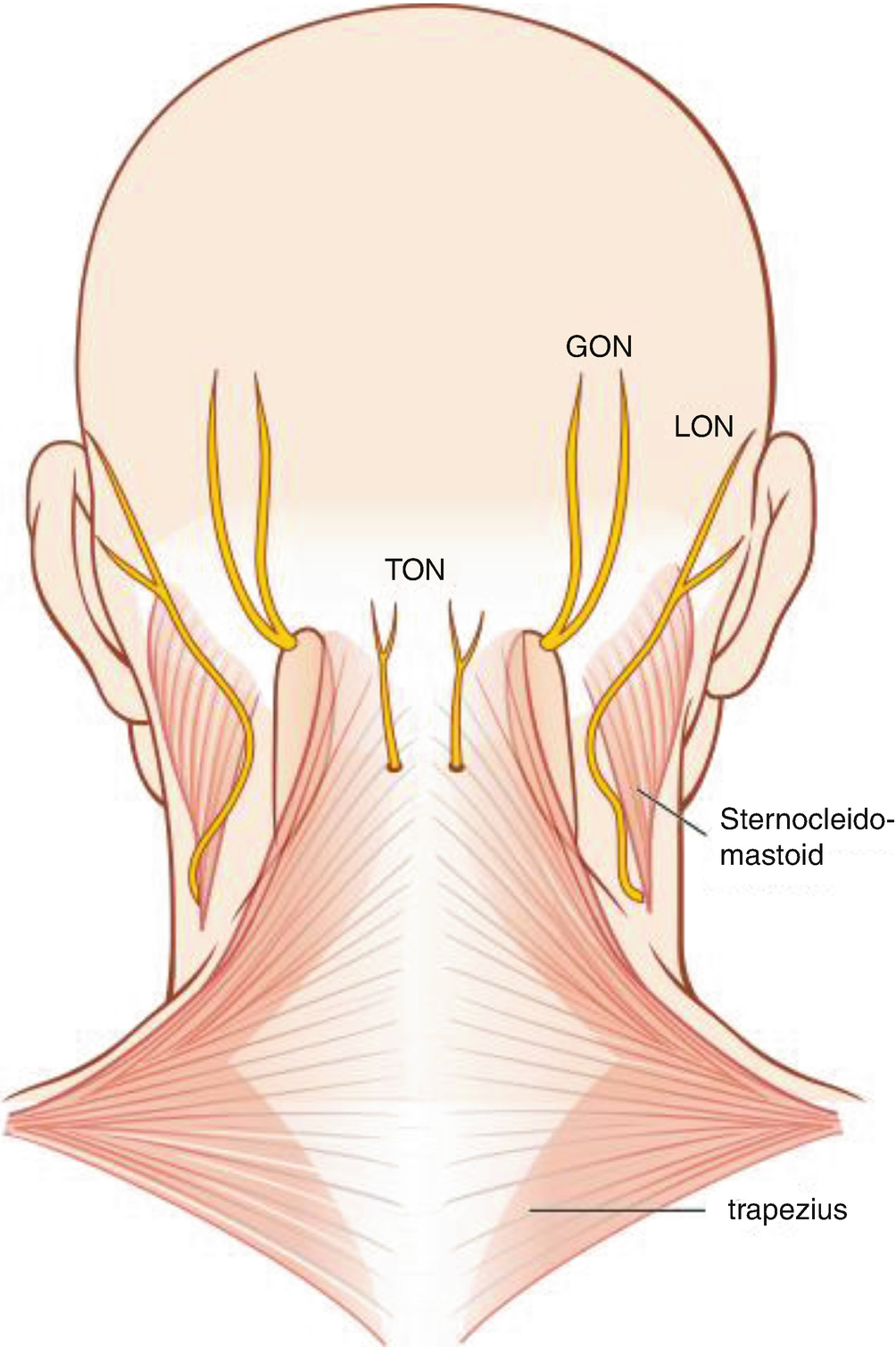
Exit points of the greater (GON), lesser (LON) and third (TON) occipital nerves (Published with kind permission of © medsteps)
The GON is the posterior ramus of a spinal nerve and arises between the first and second cervical vertebrae. The main contributions to the nerve come from the C2 spinal nerve. The GON turns dorsally and runs lateral and inferior to the obliquus capitis inferior muscle. It then pierces the underside of the semispinalis muscle, penetrates through the muscle body and exits on its surface about 3 cm below the occipital attachment of the muscle [6, 7].
Potential compression sites along the course of the GON which can cause ‘chronic inflammatory lesions’ have been described as early as 1940 [8]. The list of reported compression sites includes the pathway of its roots between atlas and axis, the perforation of the atlantoaxial membrane as well as the entry and exit point of its way through the semispinalis muscle, the trapezius muscle and its tendinous portion [9–11].
Yet, all but the last site, the aponeurotic attachment of the trapezius muscle, is rarely clinically relevant. The ‘deep’ compression sites associated with the vertebrae are important in patients with a history of trauma. The semispinalis muscle itself does not compress the nerve, though there can, infrequently, be fascial bands associated with this muscle which are wrapped around the nerve. There have been conflicting reports on whether the GON pierces the trapezius muscle. Overall, most studies found that the nerve does not run through the trapezius [2]. Aside from the usual anatomical exceptions to the rule, the semispinalis can be considered the only consistent muscular investment of the GON [12, 13] .
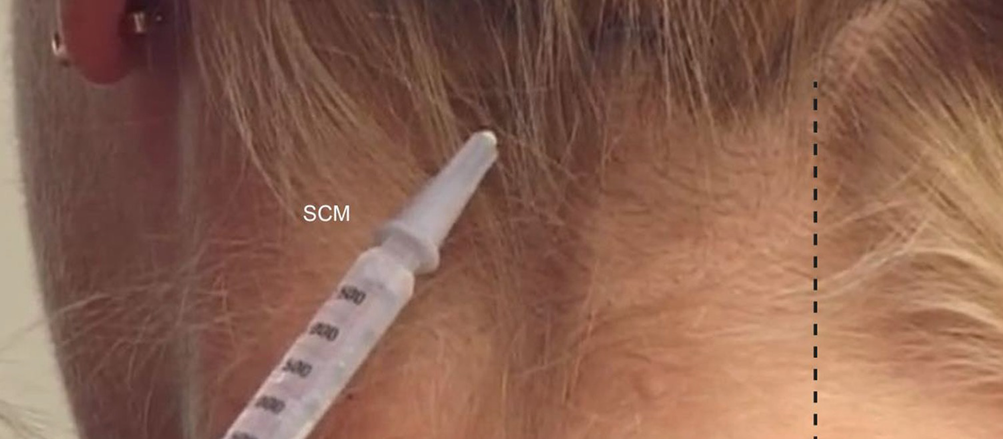
Injection site near the passage of the GON below the superior nuchal line. SCM sternocleidomastoid, dotted midline (Published with kind permission of © medsteps)
5.3 Aponeurosis
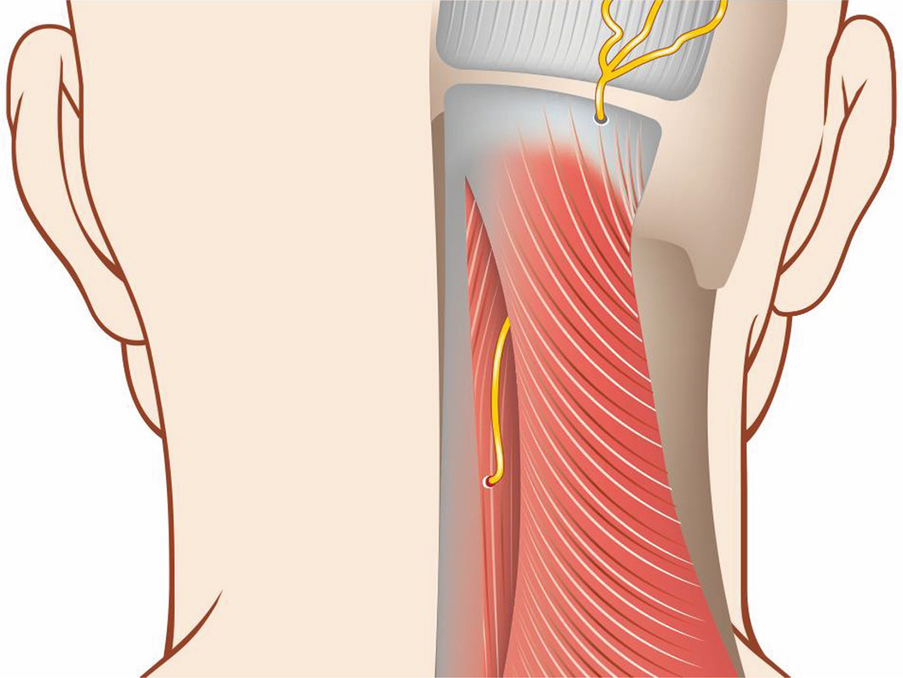
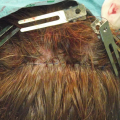
Plane of GON dissection. The trapezius muscle is incised close to the midline (Published with kind permission of © medsteps)
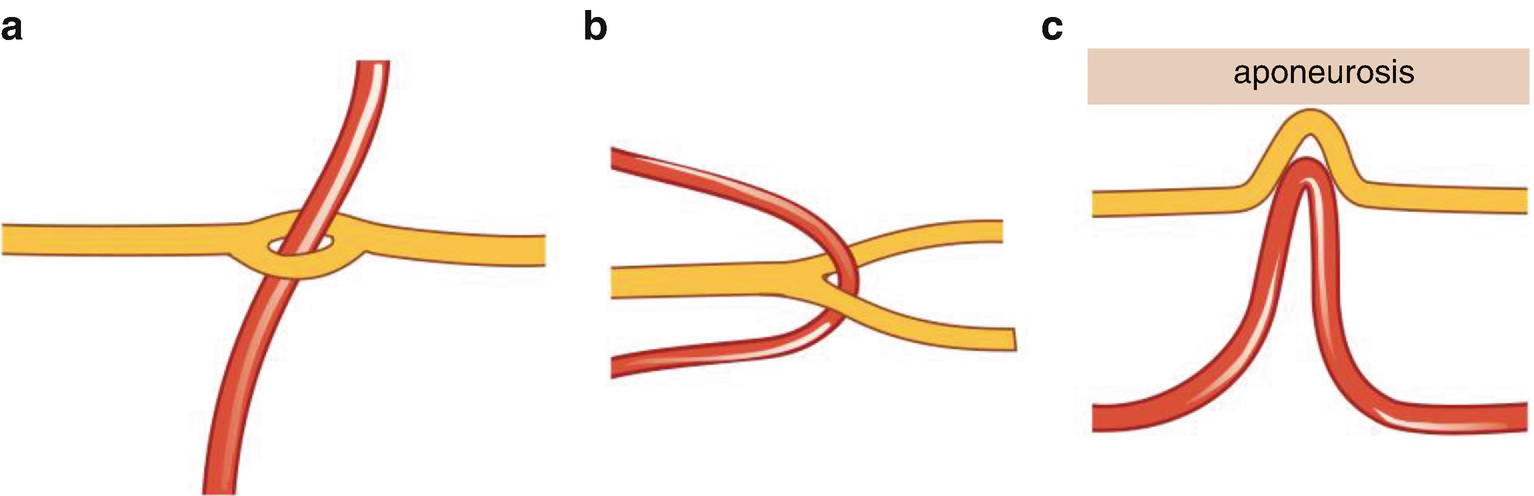
This band of aponeurotic, fibrous tissue between the highest and the superior nuchal line is the connection between the occipitalis muscle above and the occipital muscles below. The region of this band is of pivotal importance for the neck surgery in migraine patients because the penetration and compression points of the GON are located within or close to this area.
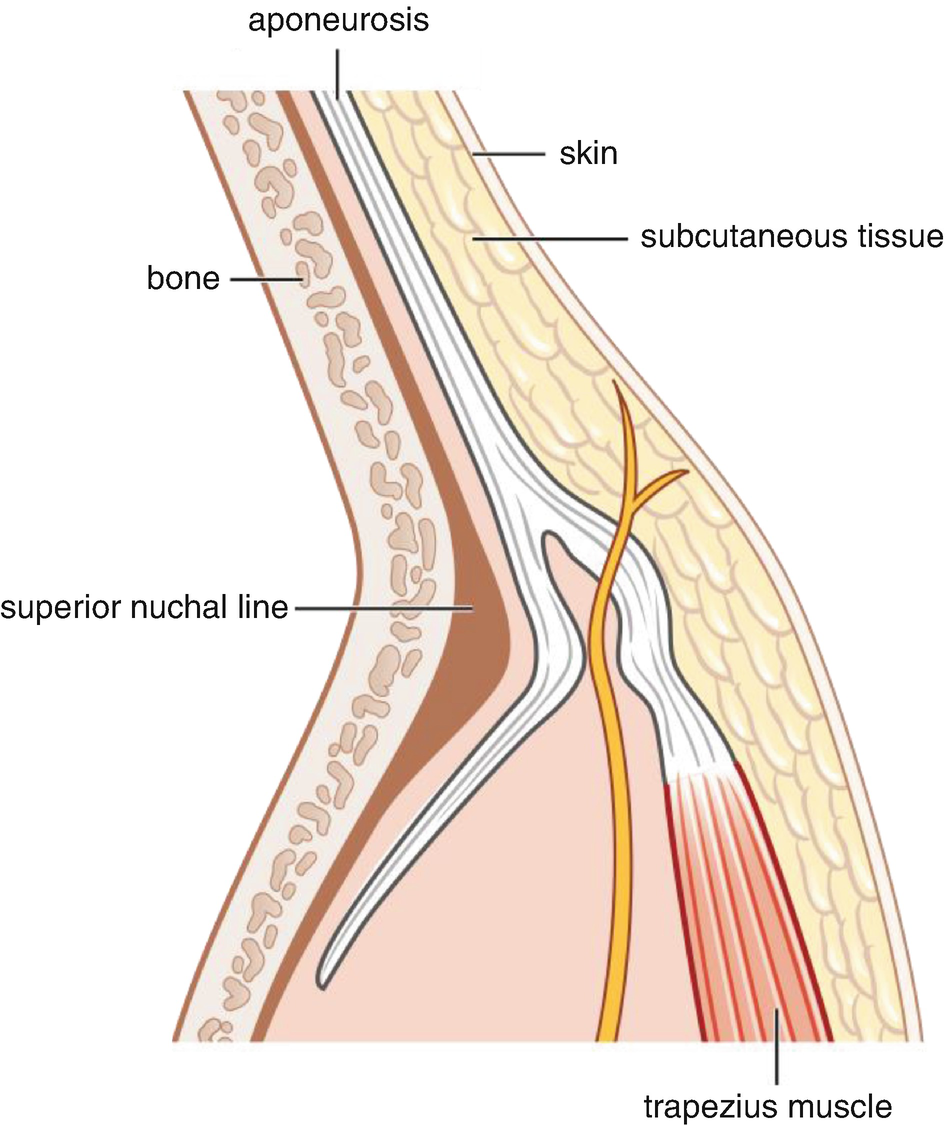
Schematic profile of the passageway of the GON through the aponeurosis (Published with kind permission of © medsteps)
The pressure on the nerve is thus not generated by muscular compression through the trapezius, but it is rather a result of the contracting muscle that is pulling the aponeurotic band downwards. In this way, the trapezius muscle can increase the pressure on the nerve by tightening the aponeurosis.
However, it is important to realize that this anatomical condition of the GON in relation to the aponeurosis is not inevitable. The nerve, albeit much more infrequently, can also pass smoothly through this area without being compressed. Instead, the pressure can be caused by a lymph node or it can originate from the occipital artery.
Related posts:
 Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
Approach for Auriculotemporal Nerve Decompression, Amirlak Modification
 Anatomy of Craniofacial Nerves Regarding Migraine Surgery
Anatomy of Craniofacial Nerves Regarding Migraine Surgery
 Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
Regional, Targeted (ART) Botulinum Toxin Injection for Migraine and Chronic Headaches
 Anatomy of the Vascularization and Innervation of the Human Scalp
Anatomy of the Vascularization and Innervation of the Human Scalp
 of Temporal Trigger Sites
of Temporal Trigger Sites
 of Occipital Trigger Sites
of Occipital Trigger Sites
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


