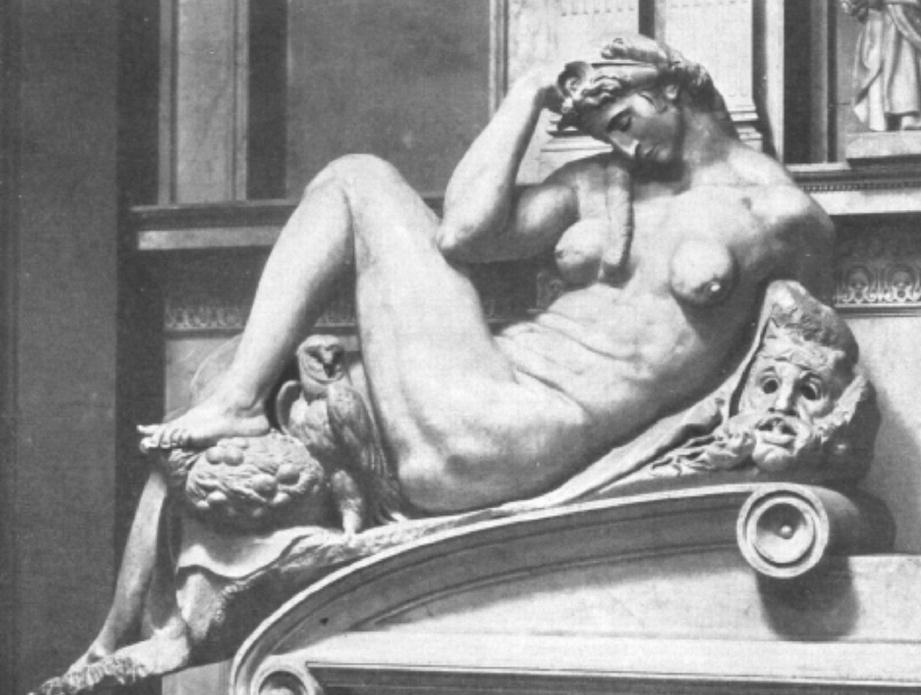
Detail of the tomb of Giuliano de Medici in Florence, Italy. Miguel Angel. (Used with permission from Schenone [46])

Currently, the importance of a woman’s breasts is manifested in the decisive influences of the mass media regarding its programming and advertising content, both of which accentuate the value of women’s breasts as a sex symbol. The glamorous look demanded by many current cultures is further enhanced by films and television [1]. The desire many women have to be physically attractive is generally accepted as a healthy sign of self-esteem, in terms of social presentation, confidence, and self-fulfillment. So important are breasts that their absence is considered a major “deformity” by many [2].
A yearning for beauty that profoundly influences humanity, especially women, combined with feelings of inferiority linked to the deformation of certain body parts and a desire to preserve one’s youthful appearance together gave birth to aesthetic surgery as an independent specialty in the 1920s.

Later, when the average life-span was longer and emphasis shifted away from a spiritual to more materialistic sphere – as in the Renaissance – the ideal woman was more large-breasted. In the twentieth century, there again were brief periods during which small breasts were fashionable: one was the 1920s and the other the late 1960s, when unisex fashions prevailed. Throughout these two periods, many women sought to assimilate with men, both professionally and economically. Since breasts were considered a defining characteristic of femininity, some women tried to hide them.
On the other hand, after the Second World War, when women with large breasts, like Marilyn Monroe, burst onto the public stage, the ideal image of women changed in many Western countries to that of domestic sexual objects born to satisfy men’s desires. It was precisely during this period when the use of augmentation mastoplasty through liquid silicone injections arose.
Following the age of unisex fashions in the 1960s and 1970s, during the conservative years marked by the United States (US) presidencies of Ronald Reagan and George Bush, big breasts once again became fashionable, and the use of mammary implants surged.
In all cultures, women have wanted to appear attractive in the eyes of men. For example, since the Chinese ascribed eroticism to small feet, many Chinese women tried to make their feet like lotus flowers by rigidly (and quite painfully) binding them. Throughout history, women have made sacrifices, often extreme, to be attractive, in accordance with the predominant model of their culture and time period. In recent years, particularly among middle- and upper-class women, anorexia and bulimia have arisen as means for women to remain thin.
Women’s desire to conform to an established image, on the other hand, exceeds their wishes to please men. In some professions—for example, among actresses and models—almost canonical adherence to beauty archetypes is required. In these fields and others, being even slightly overweight can be a major obstacle. Similarly, among women, having prominent breasts sometimes is considered a positive attribute, both personally and professionally [4].
In the modern medical age, Czerny [5] was the first to report an attempt at surgical breast augmentation through autologous tissue transplantation. Further embracing this concept, experiments were conducted employing various grafts and flaps. Failure to produce satisfactory, reproducible, and permanent results, and the limitations of autologous tissues, led clinicians to search for other materials to achieve more satisfactory breast augmentation. A wide variety of materials have been injected to modify breast contours, including high-viscosity fluids like paraffin and liquid silicones. Experiments also have been undertaken with different types of chemically altered sponge; but the subsequent hardness of these implants and their inconsistent shape made it obvious that some better solution was needed.
The introduction into the market of silicone prostheses in the early 1960s dramatically improved the results of breast augmentation and reduced the incidence of fibrous contractures and implant extrusion. At that time, all other methods previously used for breast augmentation became obsolete [45].
Methods Used to Increase Breast Volume
Among the range of techniques used to enhance breast volume, autologous tissue transplantation, injection of intramammary alloplastic materials, and preformed alloplastic implants have been the most commonly used.
Autologous Tissue Transplantation
Among the autologous tissue techniques that have been employed, two deserve historical consideration: pure fat grafts and combined tissue grafts.
According to Watson [6], the first clinical attempt to transplant fat was made by Neuber in 1893, who reported the successful use of small fat grafts in cosmetic operations involving the eye. Since larger grafts failed, Neuber recommended only using small ones.
In 1895, Czerny [5] reported the successful transplant of a lumbar region lipoma in a professional actress as a means to fill in a breast defect that had resulted from resecting an adenoma. With this procedure, Czerny performed the first augmentation mastoplasty recorded in the medical literature. He reported that the breast remained well formed, and the lipoma did not grow.
In 1917, Barlett [7] reported employing subcutaneous fat from the anterior wall of the abdomen, outer region of the thighs, and buttocks to reconstruct breasts. He recommended using a volume of fat approximately 50% greater than the breast defect that was being filled, due to “shrinkage” of the graft which he believed always occurs. He also was the first to emphasize the importance of adequate hemostasis to prevent transplant infection. In addition, he observed that the final size of a reconstructed breast typically was established by the sixth postoperative month but, also, that reconstructed breasts never achieved the consistency, firmness, or movement of a healthy breast.
Following reports published by Lexer [8] and Passot [9], fat transplantation became a widely used method for breast augmentation to treat breast hypotrophy. The method became popular even though Lexer [8], Gurney [10], and Peer [11] all claimed that fat grafts lost weight and volume over time. They argued that the transplanted volume should be considerably greater than the volume deemed necessary a priori, because only between a quarter and half of the fat graft generally survived.
May [12] found that the volume of fat that was reabsorbed was less in those patients in whom fascia was included in the graft. Subsequently, Berson [13] modified this technique and proposed fascio-dermo-lipid grafts, since incorporating the fascia and dermis, or at least one of these, appeared to reduce absorption of the fat. Moreover, such mixed tissue grafts were better protected against infection, due to enhanced capillary invasion and subsequent increased graft vitality. Bames [14] found that 90% of these three-tissue grafts survived versus just 60% of those with just dermis tissue and fat. This superiority of fascio-dermo-lipid over fat-alone grafts was later confirmed by Watson, who identified no significant graft alterations after more than 2 years of follow-up in 12 patients.
Contrary to these findings, Bouman [15] claimed that volume loss was greater with dermal-fat grafts than with fat-alone transplants. However, even Bouman sited his preference for dermal-fat transplants, because he found them easier to handle and affix and because the dermis formed a barrier against fistulas.
Although results with combined fascio-dermo-lipid grafts were promising, many surgeons retained doubts. Lewis [16] referred to the uncertainty of graft survival and the consequent reduced size and worsening asymmetry of breasts. Milward [17] was the first to warn, in 1973, about calcifications in dermal grafts, since calcification is a frequent consequence of ischemia-induced fat necrosis. In one series, for example [18], 100% of the grafts placed in 21 patients were already calcifying by the end of their fourth postoperative year. All the breasts were abnormal to palpation, including stone-hard nodules. According to Murray [18], such calcifications, by themselves, were reason enough to condemn the procedure.
With regard to composite flaps, Longacre [19] failed to observe any reduced volume among dermal flaps after 2–11 years of follow-up. His explanation for this was preservation of the extensive subcutaneous network of blood vessels.
Fascio-dermo-lipid breast augmentation transplants have since fallen into disuse [20]. However, in 1996, a technique called lipo-modeling arose among surgeons performing oncoplastic breast procedures, for use as a tool for breast reconstruction, either in association with traditional methods or as a stand-alone approach [21]. In 2013, Nava published the results of his research, from which he concluded that breast lipo-modeling doesn’t interfere with breast controls, increases the risk of neoplastic recurrence, or has carcinogenic effects per se [21].
Others have investigated the bioactivating effect of growth factors on fatty grafts. In 2007, Rigotti published his experiences with adipose stem cells and described the regenerative power of stem cells derived from adipocytes [21, 22].
Injection of Alloplastic Materials
Materials of several different origins and viscosities have been injected into breasts that have produced very poor results. In 1968, Symmers published a review of 31 patients with foreign body mastitis diagnosed between 1946 and 1967 [23]. The materials used in these patients included paraffin wax, beeswax, silicone wax, liquid silicone, lacquer, cloth of grated greased silk, silk wool, glazier putty, glass wool, and epoxy resin, with injections given in the British Isles, continental Europe, North America, and Asia. Most of the procedures were performed under aseptic techniques by doctors or cosmetologists; however, the remainder were performed by amateurs or what he termed “clandestine operators” [23].
Vaseline and Paraffin
Late in the nineteenth and early in the twentieth century, Vaseline and paraffin were injected because such injections were relatively simple and associated with little pain. In 1899, Gersuny [24] injected paraffin subcutaneously for breast augmentation, with disappointing results, due to a number of complications. In 1908, Morestin [24] claimed that his patients had to be treated for fistulas and mammary ulcers 3–8 years after being injected with paraffin. Nonetheless, by 1911, the injection of petroleum jelly and paraffin reached maximum popularity. The method was simple, painless, and appeared relatively safe. Its use became widely disseminated, though mainly in Europe and Asia, until later when local complications caused by these substances led to cessation of these procedures [25].
In 1967, Crosbie and Kaufman published a case of bilateral oleogranulomatous mastitis caused by the intramammary injection of molten petroleum jelly. The case’s relevance lies on the patient having injected herself; she had read in the nonspecialized press about Japanese women who asked doctors for this procedure and, when refused by surgeons she visited, decided to take matters into her own hands [26].
Kach et al. [27] warned that paraffin injections may yield systemic complications, like retinal, pulmonary, and cerebral emboli. The severity of the complications (which ranged from local necrosis to paraffinomas with nonmalignant paraffin metastases in the lymph nodes, patient collapse, and chronic polyarthritis) led to the disuse of this method [28]. Since then, paraffin injections have not been used by professionals.
Silicones
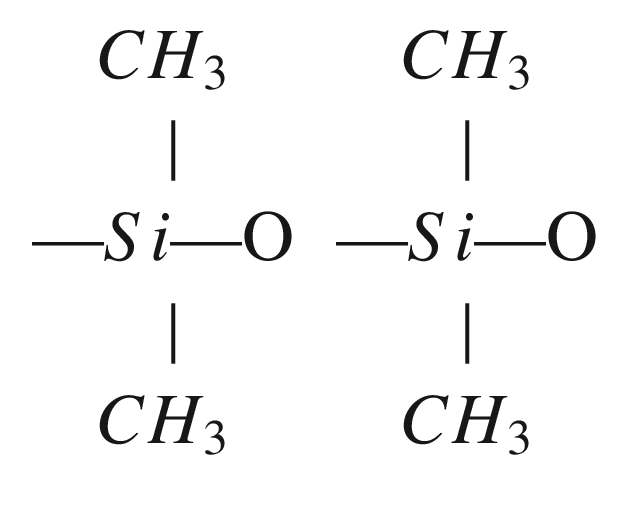
Friedel and Crafts, in 1863, were the first to synthesize a bond between silicon and oxygen, an Si-O bond, which eventually gave birth to the production of silicone polymers.
The first articles on the chemical composition of silicone were written during the first half of the twentieth century by Kipping at the University of Nottingham [29]. Silicones are a large family of polymers characterized by a chemical link between silica and both oxygen and organic groups. Silicon is a hard, black element, a solid crystal that is derived from silica or silicon oxide, SiO2. Studies conducted in the 1970s on liquid silicones revealed the presence of silica or silicon dioxide (SiO2), very widespread in nature, basically in four forms: three crystalline – quartz, tridymite, and cristobalite – and an amorphous opal, which is used in the glass industry, construction, optical lenses, building materials, ceramics, concrete, and food additives [31]. In the human body, silica has a concentration of 0.01% in connective tissue and is the essential component of glycosaminoglycans in bone, epidermis, tooth enamel, and hair [32].