With the advent of newer injectables with less immunogenicity and greater longevity, nonsurgical rhinoplasty has become a viable alternative to surgery. An understanding of the surgical anatomy of the nose, particularly in a postrhinoplasty patient, affords the physician injector the opportunity to better plan the injectable treatment. This article outlines the evolution of nonsurgical rhinoplasty and identifies properties to consider when selecting which dermal filler to use. It includes a description of the types of nasal deformities that can be treated with injectables, as well as the role of nonsurgical rhinoplasty in a comprehensive regimen for correction of nasal deformities.
Key points
- •
Nonsurgical rhinoplasty can be appropriate for patients who are reluctant to undergo surgical intervention.
- •
Effects are long lasting but not permanent.
- •
Posttreatment downtime is minimal.
- •
Calcium hydroxylapatite is the dermal filler of choice for nonsurgical rhinoplasty, because of its duration, moldability, high viscosity, and elasticity.
- •
Hyaluronic acids with high viscosity and elasticity are acceptable alternatives.
Introduction
We are in the middle of a new era of rhinoplasty, in which surgery is not the only means to address nasal defects. Nonsurgical options seem more viable than they would have been before the advent of various synthetic injectable fillers. These fillers have greater longevity and rheological properties more conducive to facial contouring than earlier nonsurgical products. As a consequence, nonsurgical rhinoplasty is becoming increasingly more popular. Many patients are now choosing to bypass permanent surgical correction in favor of a noninvasive, albeit impermanent, method for nasal recontouring.
This article outlines the evolution of nonsurgical rhinoplasty and identifies properties to consider when selecting which dermal filler to use. It includes a description of the types of nasal deformities that can be treated with injectables, as well as the role of nonsurgical rhinoplasty in a comprehensive regimen for correction of nasal deformities.
Introduction
We are in the middle of a new era of rhinoplasty, in which surgery is not the only means to address nasal defects. Nonsurgical options seem more viable than they would have been before the advent of various synthetic injectable fillers. These fillers have greater longevity and rheological properties more conducive to facial contouring than earlier nonsurgical products. As a consequence, nonsurgical rhinoplasty is becoming increasingly more popular. Many patients are now choosing to bypass permanent surgical correction in favor of a noninvasive, albeit impermanent, method for nasal recontouring.
This article outlines the evolution of nonsurgical rhinoplasty and identifies properties to consider when selecting which dermal filler to use. It includes a description of the types of nasal deformities that can be treated with injectables, as well as the role of nonsurgical rhinoplasty in a comprehensive regimen for correction of nasal deformities.
The evolution of nonsurgical rhinoplasty
Initial reports of injectable contouring or nonsurgical rhinoplasty date back to the middle of the 1980s. At the time, treatment options were limited to bovine collagen and silicone. However, since that time, semipermanent dermal fillers have increasingly been noted in the literature as acceptable formulations for nonsurgical rhinoplasty. Although use of dermal fillers in nonsurgical rhinoplasty remains an off-label application of hyaluronic acids (HA) and calcium hydroxylapatite (CaHA), their use in correction of nasal deformities has been widely reported in the clinical literature over the years, as shown in Table 1 .
| Reference | Filler/Procedure | Key Points of Study |
|---|---|---|
| Knapp and Vistnes, 1985 | Bovine collagen/surgical depressions resulting from rhinoplasty | Short-term filler may retain correction indefinitely |
| Webster et al, 1986 | Medical grade silicone/injected subdermally for postrhinoplasty defects | 347 patients/1937 treatments; recommended undercorrection because filler stimulates indigenous collagen growth |
| Han et al, 2006 | Restylane (Q-Med, Uppsala, Sweden) coupled with autologous fibroblasts from harvested dermis/augmentation rhinoplasty | 11 patients; 10%–40% resorption in the first 6 mo in 6 patients; stabilization at 6 mo. Minor surgery rather than noninvasive as a result of epidermal flap necessary for harvesting. Used fibroblasts to increase longevity |
| Beer, 2006 | Restylane/postrhinoplasty defect of nasal dorsum | Case report of 1 patient: safe, inexpensive, well-tolerated; mention of CaHA as alternative |
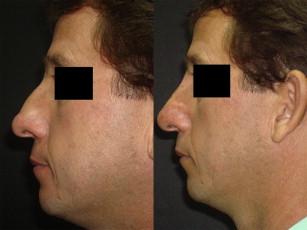
| Becker, 2006 | Radiesse (Merz Aesthetics, San Mateo, CA)/Nonsurgical rhinoplasty | 25 patients, 15 with previous surgical rhinoplasty; viable alternative to surgery; preferred CaHA caused by moldability and durability; mean patient satisfaction 7.9/10 |
| Rokhasar and Ciocon, 2008 | Radiesse/primary correction of nasal deformities | 14 patients; no significant complications, high patient satisfaction |
| De Lacerda and Zancannaro, 2007 | Porcine collagens and HAs/filler rhinoplasty vs augmentation rhinoplasty | Filler rhinoplasty perhaps more accurate term than augmentation because of creating illusion of smaller nose through augmentation |
| Cassuto, 2009 | Evolence (Ortho Dermatologics, Skillman, NJ)/nonsurgical rhinoplasty | 12 patients; mean follow-up of 8 mo with stable correction |
| Siclovan and Jomah, 2009 | Evolence/nasal deformities and postrhinoplasty irregularities | Correction for up to 1 y |
| Humphrey et al, 2009 | HAs, CaHA, silicone review article | HA/CaHA safest available agents for nasal dorsum and sidewall deformities. Caution against filler in tip of nose |
| Rivkin and Solieman-zadeh, 2009 | CaHA in nonsurgical rhinoplasty | 4-y retrospective study of 385 patients (295 for follow-up). 46% required touch-up 2 mo after initial treatment; 28% touch-up 2–6 mo after initial treatment; 18% touch-up 6 mo to 1 y after initial treatment. AE: prolonged erythema (more prevalent in postsurgical rhinoplasty patients) with 2 cases of partial skin necrosis and 6 cases of cellulitis |
| Bray et al, 2010 | Restylane/nonsurgical nasal augmentation and postrhinoplasty asymmetry | Duration up to 18 mo; mention of CaHA to treat internal valve collapse |
| Dayan and Kempiners, 2005 | Botulinum toxin either alone or with injectable fillers/nasal tip ptosis and acute nasolabial angle | 5 units of botulinum toxin in depressor septi muscle bilaterally and 3 units into each levator labii superioris alaeque nasi muscle |
| Monreal, 2011 | Autologous fat transfer/stand-alone correction or with surgical rhinoplasty | 33 patients, 36 treatments; grafting to radix, glabella, pyriform aperture. Volume decrease first 15–30 d, stable thereafter. Duration unknown |
| Kim and Ahn, 2012 | Radiesse/nonsurgical augmentation in Asian population | 87 patients, 4 complications: 1 dorsal asymmetry (corrected), 1 overinjection of columella-labial angle causing intraoral submucosal nodule, 1 self-limited dermatitis, 1 inflammation/erythema at injection site; plane was subdermal with CaHA and intradermal with HA for tip |
Selecting the appropriate filler for nonsurgical rhinoplasty
The available choices of fillers for nonsurgical rhinoplasty primarily include cross-linked HA products (Restylane [Medicis Aesthetics, Scottsdale, AZ], Perlane [Medicis Aesthetics, Scottsdale, AZ], Juvederm Ultra [Allergan, Irvine, CA], and Juvederm Ultra Plus [Allergan, Irvine, CA]) and CaHA (Radiesse [Merz Aesthetics, San Mateo, CA]). The 2 most commonly used fillers for injectable rhinoplasty seem to be Restylane and Radiesse, based on a review of the available literature. Although most investigators do not explain the rationale behind their selection of 1 filler rather than another, several physicians have included explanations for their choice of dermal filler. Becker made reference to the moldability of Radiesse in his report; Rokhsar and Ciocon expressed a preference for Radiesse because of its durability as a subcutaneous filler and its lack of immunogenicity, obviating skin testing.
Assuming safety as a given in temporary fillers available in the United States, when selecting a filler for nonsurgical rhinoplasty, various factors are considered. In our clinical practice, we choose fillers based on their properties of longevity, viscosity, elasticity, and degree of hydrophilicity. We prefer a filler that is not permanent but instead one that is long lasting and semipermanent. Silicone (off-label) and Artefill are the 2 permanent fillers currently available in the United States. Although the concept of permanence is intriguing, it does bring into play the long-term sequelae such as granulomas and additional hindrances to any surgical revisions.
Two important qualities in a filler are viscosity (n*) and elasticity (G′).
Viscosity refers to the ability of the gel to resist sheering forces. Viscosity is the ability of a material to resist a force applied to it, which means that it is less likely to spread. Lower viscosity products are more easily spread and high n* products tend to stay put, making for more precise sculpting.
Elasticity is a measure of the ability of the material to resist deformation when pressure is applied. A higher G′ filler provides more lift and support and requires smaller volumes to achieve correction.
Fillers with high n* and high G′ are particularly desirable for nonsurgical rhinoplasty. Sundaram and colleagues studied the rheological properties (viscosity and elasticity) of 6 cross-linked HA products (Restylane, Restylane Sub-Q [Q-Med, Uppsala, Sweden], Perlane, Juvederm Ultra, Juvederm Ultra Plus, and Juvederm Voluma [Allergan, Pringy, France]), in addition to CaHA and CaHA mixed with lidocaine as per US Food and Drug Administration guidelines. Based on these investigators’ data, the products fell into 3 groups: undiluted Radiesse was in the high n* and G′ category. Radiesse mixed with 0.3% lidocaine and 3 HA products (Restylane, Perlane, and Restylane Sub-Q [not available in United States]) were in the medium group. The other HAs studied (Juvederm Ultra, Juvederm Ultra Plus, and Juvederm Voluma [also not available in the United States]) were in the low n* and low G′ group.
The n* and G′ of each product can be altered by diluting it with lidocaine or saline, an increasingly popular strategy. However, overdilution may lead to the need for increased product being injected at the target site. Being able to produce contour changes with very small volumes is advantageous, so caution is recommended regarding dilution of the inherent product of the dermal filler because larger volumes of injectate may lead to a higher incidence of adverse vascular events.
Hydrophilicity is another factor to consider. There are times when the hydrophilic effect of HA products is desirable. From our clinical perspective, and that of others as well, the hydrophilic effect may be disadvantageous in filler rhinoplasty. The expansion that occurs with the influx of water into the tissues may increase the potential for compression of dermal and subdermal vessels, possibly thereby leading to vascular compromise. Of the HAs, Restylane and Perlane are less hydrophilic than Juvederm Ultra and Ultra Plus.
In our clinical practice, CaHA is the filler of choice for nonsurgical rhinoplasty. Its properties approach those of an ideal filler for this particular application, specifically its longevity (averaging roughly 9–12 months) and its moldability. However, the reversibility of HA products with hyaluronidase makes them attractive to many, especially for aesthetic physicians with less experience in nonsurgical rhinoplasty.
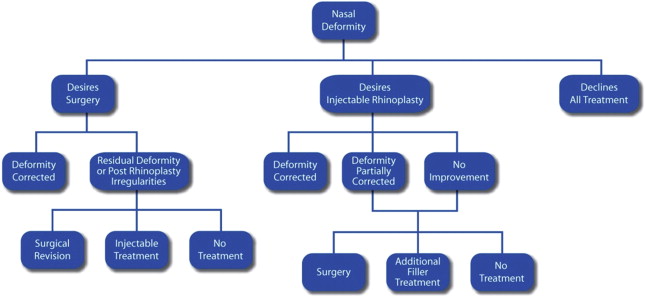
Indications for nonsurgical rhinoplasty
A well-considered treatment plan is an essential element in any patient’s course of care. To that end, a treatment algorithm has been provided in this article to help physicians when discussing surgical and nonsurgical options ( Fig. 1 ). Nonsurgical rhinoplasty is a comprehensive term for the subject of nasal defect corrections. Specific nasal areas of corrective treatment through nonsurgical means include hump removal, deep radix, side wall deformities, tip projection, tip rotation, dorsal augmentation, nasal lengthening, columella retraction, nasolabial angle, saddle nose, contour irregularities, and asymmetry.
Pretreatment anesthesia
Anesthetizing the nose is an important step in nonsurgical rhinoplasty. If the patient is comfortable during the injection session, they are likely to return for future sessions or refer others for treatment. Topical anesthesia consisting of lidocaine 5% is applied to the nose for approximately 30 minutes. Using 1% lidocaine with 1:100,000 of epinephrine, the infratrochlear and infraorbital nerves are blocked. Rather than blocking the entire infraorbital nerve, the medial branches are anesthetized by infiltrating along the frontal process of the maxilla (approximately along a line where a low lateral osteotomy would be performed). The anterior superior alveolar nerve is blocked intraorally, with the local anesthesia being injected at the anterior nasal spine (application of topical anesthesia to the oral mucosa around the frenulum makes this more comfortable). If no tip or columellar work is planned, the anterior superior alveolar nerve block may be deleted. If the physician is concerned with excessive vasoconstriction of the nasal tip, plain lidocaine should be considered.
Injection guidelines
Although the sequence of injection of CaHA (or any dermal filler) varies depending on the deformity to be treated, certain steps are common to all nonsurgical rhinoplasties. For example, a concerted effort should be made to create all entry points distant from the injection site. Distant entry, from a lateral perspective along the dorsum with placement of a series of small boluses (0.1 mL or less), helps avoid tissue edema and distortion of the target site, which could occur as a result of multiple punctures and passes of the needle.
Sometimes, a static bolus method is deployed; at other times, a moving bolus with a retrograde injection is the method of choice. This moving bolus is a hybrid between a static bolus and linear threads, which fills the dorsum from 1 dorsolateral junction to the other, thereby avoiding the dorsum from looking too thin as a result of the placement being just in the midline.
Particularly in the tip or ala, avoidance of injection of a filler under pressure is prudent, in no small part to prevent vascular occlusion. When treating the tip, some degree of subcision is usually performed using the 27-gauge, 3.17-cm (1.25-inch) or 28-gauge, 1.9-cm (0.75-inch) needle used for the injection. Boluses in the tip are very small (0.05 mL or less). The injection plane is deep-supraperichondrial or supraperiosteal. A lateral angle of entry is preferred, but other angles may be used as needed.
Dorsal Hump and Low Radix
One of the most common reasons for which patients present for nonsurgical rhinoplasty is correction of a dorsal hump ( Figs. 2 and 3 ). A hump typically comprises bony and cartilaginous elements. Begin treatment of a hump by first injecting above the hump from the superior extent of the hump upward to the radix. This procedure usually entails some filling of the nasofrontal angle. Attention to this area is important to avoid overfilling the angle and thereby inadvertently producing an unnatural straight-line deformity from the forehead down to the hump. A low radix as an isolated problem is treated in similar fashion to a dorsal hump. The more inferior aspect of the radix is filled first and the injection then proceeds cephalad until correction is complete ( Fig. 4 ).
- •
Entry is from the lateral aspect of the nose just below the junction of the nasal dorsum and lateral aspect of the nasal bone (dorsolateral junction), beginning just above the hump.
- •
The needle or cannula is positioned in a supraperiosteal plane and advanced to the opposite dorsolateral junction by walking the tip of the needle along the periosteum.
- •
The position of the needle tip is monitored by palpation with the index finger of the nondominant hand.
- •
Gentle subcision is carried out and the needle withdrawn to the midline, remaining in a supraperiosteal plane.
Procedure note: advancing the needle beyond the midline helps to create a space that allows for the filler to expand to the contralateral side, not just ipsilaterally in the direction of the entry point.
- •
A bolus of approximately 0.1 mL or less is then injected, depending on the size of the hump.
Procedure note: in general, it is always prudent to err on the conservative side when judging bolus volumes. However, most overcorrections can usually be remedied with molding and massage if the overcorrection is not too severe. Indeed, 1 of the reasons that CaHA is the preference for this procedure is that it can be easily molded into the desired configuration while maintaining its new shape, rather than splaying into the tissues. Keeping injection in the proper supraperiosteal or supraperichondrial plane also helps to facilitate the molding process.
- •
This process is continued by extending upward from the superior extent of the hump to the nasofrontal angle.
- •
The correction above the hump is then reassessed and supplemental injections or additional molding are carried out as indicated.
- •
The area of the dorsum inferior to the hump is then addressed.
- •
Once the dorsal hump correction is completed, the nasal tip is then assessed to see if there is need for increased tip projection (to preserve or create a supratip dip) or the illusion of tip rotation.
- •
The columella and nasolabial angle should also be inspected to help ensure that all areas of the nose are brought into proper harmony.