With increasing interest in facial rejuvenation procedures, it is critical to consider concomitant restoration of the anterior neck to achieve a natural-looking, cohesive esthetic. Numerous nonsurgical modalities may be used alone or in combination to correct neck skin dyspigmentation, laxity and rhytids, platysmal banding, submental fat accumulation, and jowling.
Key points
- •
With increasing interest in facial rejuvenation procedures, it is critical to consider concomitant restoration of the anterior neck to achieve a natural-looking, cohesive esthetic.
- •
Aging of the neck is a multifactorial process that leads to skin dyspigmentation, progressive laxity and rhytids, platysmal banding, submental fat accumulation, and jowling.
- •
Compared to facial skin, the neck has a thinner epidermis and dermis, less subcutaneous fat, and fewer pilosebaceous units, all of which contribute to slower healing and increased risk for resultant complications from treatment.
- •
Skin dyspigmentation can be addressed with laser and light-based technologies, whereas correction of laxity and rhytids often requires a combination approach using radiofrequency, microfocused ultrasound, dermal fillers, and injectable biostimulators.
- •
Cryolipolysis, chemical lipolysis, and laser lipolysis are all beneficial in the reduction of submental fat.
Introduction
Although the gold standard treatments for neck skin laxity and submental fat accumulation remain lower rhytidectomy and liposuction, respectively, these surgical procedures are associated with increased morbidity and downtime that may not be appealing or appropriate for some patients. Nonsurgical neck rejuvenation is an area of significant growth with numerous innovations to address skin dyspigmentation, laxity and rhytids, platysmal banding, and submental fat accumulation. These minimally invasive interventions may provide significant cosmetic benefits while minimizing downtime and unwanted side effects. Because the anterior neck is contiguous with the lower one-third of the face, it is imperative to discuss rejuvenation of the neck as a complementary procedure when seeing a patient in consultation for facial rejuvenation.
Neck anatomy and aging
Anatomy of the Anterior Neck
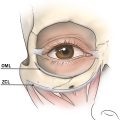
The neck can be divided into anterior and posterior triangles; however, our discussion of nonsurgical neck rejuvenation will focus specifically on the anterior neck. Bounded inferiorly by the sternal notch and clavicles, bilaterally by the sternocleidomastoid muscles, and superiorly by the chin and lower mandibular line, the anterior neck anatomically transitions to the lower third of the face and is fundamental to the overall facial esthetic [ ]. From superficial to deep, the anterior neck is composed of skin, subcutaneous fat, platysma muscle, and underlying fibrous fascia [ ]. The interplay of underlying structures and the skin’s quality and ability to drape atop is what contributes to the perception of a youthful or aged neck. It is important to recognize that compared to facial skin, the neck has a thinner epidermis and dermis, less subcutaneous fat, and fewer pilosebaceous units, all of which contribute to slower healing and a higher risk of resultant complications secondary to treatment [ ].
Aging
With increasing interest in facial rejuvenation procedures, it is critical to consider concomitant restoration of the anterior neck to achieve a natural-looking, cohesive esthetic. Previously described criteria for an esthetically pleasing neck include a distinct mandibular border, a cervicomental angle of 105° to 120°, a visible anterior border of the sternocleidomastoid, an appreciable subhyoid depression, and an apparent thyroid bulge [ ].
Just as in the aging face, the skin of the anterior neck is not only subject to chronologic aging but also affected by chronic photodamage. Cumulatively, these intrinsic and extrinsic factors lead to skin dyspigmentation, progressive laxity and rhytids, platysmal banding, submental fat accumulation, and jowling. Of note, the neck is particularly susceptible to gravitational descent, which is largely attributable to volume loss in the face. Therefore, volume replacement in the midface and lower face may be necessary to provide structural support to improve the appearance of redundant, lax neck skin.
Skin dyspigmentation
Intense Pulsed Light
Intense pulsed light (IPL) devices emit a broad spectrum of wavelengths (400 nm–1200 nm) and are effective in the treatment of photodamage characterized by mottled brown pigmentation, diffuse erythema, and telangiectasias, also known as poikiloderma of Civatte. Goldman reported a 50% to 75% improvement in the extent of hyperpigmentation and telangiectasias on the neck after an average of 2.8 IPL treatments performed at various settings every 4 weeks until desired improvement was observed [ ]. Although IPL often requires multiple treatments, the minimal downtime and low risk of adverse effects make it an appealing therapeutic option for dyschromia and vascularity of the anterior neck. When compared with other light-based energy devices, IPL has a higher learning curve with an increased number of variables—including filters, pulse duration, fluence, and the ability to double or triple pulse—making it more user dependent and prone to complications, such as edema, bullae formation, crusting, hyper/hypopigmentation, scarring, keloid formation, and infection. In general, IPL is not considered safe in patients with darker Fitzpatrick skin types because it has difficulty distinguishing hyperpigmentation and vascularity from physiologic, melanin-rich skin and may therefore cause pigmentation problems to worsen.
Quality-switched and Picosecond Lasers
Use of quality-switched (QS) lasers, with energy pulses in the nanosecond range, and picosecond (PS) lasers, with energy pulses in the PS range, enable energy to be deposited very quickly to selectively target the small melanin particles comprising pigmented lesions while minimizing collateral thermal damage to the normal surrounding tissue [ ]. Vanaman suggests the combined use of IPL followed by same-day QS 532, 694, or 755 nm laser to selectively target pigmented macular seborrheic keratoses or light lentigines on the neck, prevents the need to increase one’s IPL settings [ ]. Additionally, the 755-nm PS pulsed alexandrite laser with diffractive lens array (DLA) has shown efficacy in the treatment of dyspigmentation, keratoses, and skin texture of the face and neck [ ] as well as the décolletage [ ]. The addition of the DLA handpiece to the 755-nm PS laser allows for superficial targeting through a hexagonal lens array that delivers 70% of the total energy through microspots, with the remaining 30% distributed in a low-fluence background. These focal zones of concentrated energy generate microthermal zones of destruction in the epidermis to treat fine lines and wrinkles [ ]. Potential complications from use of QS and PS lasers include pigmentary alteration, thermal injury, and scarring. Some of these risks may be mitigated by using pretreatment and posttreatment topical bleaching cream (4%–5% hydroquinone compounded with 1%–2% hydrocortisone and 0.05%–0.1% tretinoin), use of a large spot size, and appropriate spacing of treatments at 6 to 8 weeks.
Skin laxity and rhytids
Nonablative and Ablative Fractional Resurfacing
Nonablative and ablative fractional lasers are also effective in the treatment of dyschromia on the neck with the added benefit of improving laxity and rhytids. In fractional photothermolysis, light energy creates discrete microscopic zones of thermal damage that extend into the reticular dermis without affecting intervening skin. The adjacent columns of undamaged tissue serve as reservoirs for rapid wound healing, limiting recovery time when compared to traditional ablative resurfacing. Nonablative fractional photothermolysis induces columns of necrosis within the epidermis and dermis while leaving the skin intact, whereas ablative fractional photothermolysis vaporizes the targeted microthermal zones and is therefore a more aggressive treatment option that can confer a greater risk profile. Because of this, some physicians prefer to use the safer nonablative fractional laser on the neck to prevent adverse events such as scarring and dyschromia; however, this can require more treatment sessions to achieve similar efficacy as ablative fractional resurfacing.
A recent study compared the efficacy and safety of radiofrequency microneedling (RFMN) versus a nonablative fractional 1550-nm erbium:glass laser for neck rejuvenation, concluding patients who received 3 nonablative fractional treatments 4 weeks apart had significantly better subject satisfaction and blinded investigator wrinkling and elastosis scores than those treated with the same number of RFMN sessions [ ]. Another study evaluated the utility of a nonablative fractional 1540-nm erbium:glass laser in the treatment of aged neck skin and reported 6 laser treatments performed at 4-week intervals demonstrated significant clinical improvement of dyschromia and wrinkles but was not effective for the laxity of the neck skin [ ].
Oram evaluated the use of ablative fractionated laser resurfacing on the neck of 20 patients with Fitzpatrick skin types II to IV and reported sustained improvement in skin laxity, jowling, fat deposition, and horizontal neck lines at 1 month and 1 year posttreatment. Anesthetic cream (EMLA, eutectic mixture of 2.5% lidocaine and 2.5% prilocaine) was applied under occlusion for 1 hour before patients underwent a single pass with the 10,600 nm fractional CO 2 laser (Candela QuadraLase, Candela, Wayland, Massachusetts) using a 300-μm handpiece attachment, 12 to 14 W energy, 3.5 millisecond pulse width, and 20% to 30% coverage (approximately 200–250 μm depth). The overall complication rate was 35%; however, these adverse events, which included short-lasting erythema, edema, epidermal bronzing, crusting, exfoliation, infection, and postinflammatory hyperpigmentation, were all transient. Nevertheless, one should demonstrate caution when treating the neck with ablative lasers given its tendency to develop hypertrophic scarring after thermal injury [ ].
Several studies have also documented the utility of combining other treatment modalities, such as RF and microfocused ultrasound (MFU), with use of nonablative [ ] and ablative fractionated laser [ ] therapy for synergistic effects.
Radiofrequency
Radiofrequency (RF) technology has emerged as a noninvasive treatment of esthetic rejuvenation of the face and neck. Mechanistically, heat is generated from the natural impedance of tissue to the movement of electrical current generated by RF devices. Consequently, this thermal energy induces injury to the dermis and subcutaneous fat, resulting in dermal collagen contraction, neocollagenesis, and apoptosis of adipocytes.
Numerous studies have reported the safety and efficacy of various monopolar RF devices for the improvement of neck skin laxity [ , ]. In monopolar RF, high-frequency electrical current passes through a single electrode in the handpiece and returns to a grounding pad on the patient’s body. The heating of the dermis and fibrous septae is associated with immediate collagen denaturation resulting in subsequent thickening and shortening of the collagen fibers, increased fibroblast activity, and new collagen formation that objectively produces skin tightening during 4 to 6 months [ ]. Improvement in neck skin laxity can be seen after just one treatment ( Fig. 1 ). However, a limitation of transcutaneous monopolar RF is the inability to deliver consistent and measurable temperatures to the level of the subcutaneous fat without overheating the epidermis, which prevents deeper collagenous tissue remodeling and sufficient apoptosis of adipocytes. Complication rates from monopolar RF are generally low, however, transient edema, erythema, and dysesthesia, often in the distribution of the greater auricular nerve, have been observed. Without adequate epidermal cooling, there is also a risk of thermal burns and subsequent scarring.

In response, a thermistor-controlled subsurface monopolar RF device (ThermiTight; ThermiAesthetics, Irving, TX) has emerged, which uses a percutaneous probe to administer RF directly to dermal and subdermal tissue. A retrospective study of 35 patients who underwent ThermiTight for submental skin tightening demonstrated significant improvement in laxity 30 days after the procedure [ ]. Subsurface monopolar RF devices have been anecdotally associated with a higher incidence of edema and bruising when compared to externally applied monopolar RF devices, likely because of preprocedural local anesthetic infiltration. Additionally, there have been reports of transient marginal mandibular nerve palsies after jowl treatment [ ].
More recently, the use of fractional insulated RFMN has been used as a treatment modality for skin laxity of the neck with the added benefit of addressing submental fat accumulation. This technology uses microneedles with insulated shafts and exposed tips to deliver precise RF energy to the deeper subcutaneous tissues to enhance adipocyte apoptosis. The sheathed configuration of the needle and exclusive delivery of RF at the noninsulated distal portion limits epidermal damage to mechanical microneedling and obviates epidermal cooling. Clementoni treated 33 patients with mild-to-moderate skin laxity of the lower face/neck with 3 fractional insulated RFMN treatments at monthly intervals, administering 3 passes per session with decreasing dermal depths for each pass, and reported a significant posttreatment decrease in the cervicomental (28.5°) and gnathion angles (16.6°) [ ]. Furthermore, a recent study of 30 patients who received 1 to 3 sessions of fractional insulated RFMN treatments (Genius; Lutronic Medical Systems, Hamburg, Germany) to the lower face, jawline, and neck region exhibited a mean submental volume difference of −4.72 cm 3 and most patients were very (65%) or mainly (95%) satisfied on Day 180 posttreatment [ ]. An additional study evaluating a novel fractional RF device with microinsulated needles in 24 patients reported a 19.72% decrease in the quantitative volume change of the submental fat 2 months after a single treatment [ ]. In general, fractional insulated RFMN is well tolerated and safe in darker Fitzpatrick skin types. The most commonly observed adverse events include transient PIH and erythema in a grid-like distribution [ ].
Microfocused Ultrasound
In addition to laser devices and RF, MFU has emerged as an effective means for tightening and lifting lax skin of the face and neck. MFU produces small (∼1 mm 3 ) zones of thermal damage by heating tissue to ∼60°C at predetermined depths of 1.5, 3.0, and 4.5 mm deep, which spares the overlying papillary dermis and epidermis. This focused fractionated heating of mid to deep reticular dermal collagen induces neocollagenesis and clinically results in skin tightening and lifting of lax skin. MFU with visualization (MFU–V) describes an MFU device combined with high-resolution ultrasound imaging that is used to visualize the treated tissue and ensure proper acoustic coupling. A retrospective study of 48 patients who received a single MFU–V treatment of the face and upper neck using the 4-MHz, 4.5 mm and 7-MHz, 3.0-mm depth transducers (Ulthera System; Ulthera, Inc., Mesa, AZ) reported 81.3% and 77.7% of patients achieved improvement at Day 90 and 180, respectively [ ]. When compared with subsurface monopolar RF, MFU was equally effective, and there were no statistical differences in measures of neck laxity, patient satisfaction, or adverse events [ ]. MFU–V has an excellent safety profile with the most reported adverse events including mild erythema, edema, bruising and tenderness, and dysesthesia or numbness. Uncommon events include pseudofacial fat atrophy and elevated wheals or white linear striations of the neck, which may be attributable to improper transducer coupling [ ].
Synchronous Ultrasound Parallel Beam
High-intensity, high-frequency Synchronous Ultrasound Parallel Beam (SUPERB) technology is another ultrasound-based procedure that is Food and Drug Administration (FDA) approved for wrinkle improvement, as well as for eyebrow, neck, and submental lifting treatments. Compared with MFU, which delivers energy at 1.5 mm, 3.0 mm, and 4.5 mm, the SUPERB device produced by Sofwave Medical Ltd. (San Clemente, CA) only delivers energy at a depth of 1.5 mm, exclusively targeting the mid-dermis. Each pulse of the Sofwave device delivers high-intensity energy from all 7 parallel beam transducers in the handpiece, inducing three-dimensional cylindrical volumetric thermal zones that extend into the mid-dermis and stimulate collagen and elastin remodeling without disrupting the epidermis or causing damage to underlying nerves, blood vessels, or adipose tissue. The integrated cooling system in the handpiece protects the epidermal layer; however, skin blistering and thermal burns remain potential complications. Although SUPERB technology is considered more tolerable and timesaving than MFU, limiting the depth of thermal damage to 1.5 mm prevents remodeling of the reticular dermis and superficial musculoaponeurotic system that is achievable with the 3.0 mm and 4.5 mm MFU transducers [ ].
Hyaluronic Acid Fillers
Hyaluronic acid (HA) fillers with low viscosity and elasticity are most often used for the treatment of horizontal neck rhytids due to their properties of being soft and easily molded. Rongthong described the treatment of 30 patients with one session of HA filler injections (Belotero Balance; Merz Aesthetics, Raleigh, NC) to treat horizontal neck lines by blunt cannula injection technique. All subjects received approximately 3 mL of HA fillers for the entire treatment area and results demonstrated peak improvement at 1 month but with sustained rejuvenation effects up to 6 months after treatment [ ].
In contrast to the blunt cannula technique, Lee described the safe and efficacious use of a 0.3-mL insulin syringe with a 31 G × 8 mm needle for the treatment of horizontal neck lines using either monophasic (Belotero Balance; Merz Aesthetics, Raleigh, NC) or biphasic (Restylane Vital; Q-Med AB, Uppsala, Sweden) HA filler, injected by the linear threading technique (LTT) and vertical technique (VT). In the LTT, the needle is inserted into the horizontal neck lines and 0.02 to 0.04 mL of filler material is injected into the deep dermis over a length of 8 mm to create columns parallel to the skin surface. Each injection is spaced approximately 1 cm apart and manual molding with a cotton-tipped applicator is performed after every 3 to 5 injections. In the VT, the needle is inserted into the horizontal neck lines and 0.01 to 0.02 mL of filler material is injected into the deep dermis per point with injections spaced at an interval of 0.5 cm apart. After 5 to 10 VT injections, the round and vertically positioned pouches are manually molded to merge into a continuous band of subwrinkle support [ ].
Poly- l -lactic Acid
Poly- l -lactic acid (PLLA; Sculptra, Galderma, Fort Worth, TX) is a synthetic, biodegradable, injectable soft tissue biostimulator that produces gradual volume restoration by stimulating local fibroblasts to promote neocollagenesis. Traditionally used in the treatment of human immunodeficiency virus-associated lipoatrophy, PLLA has gained utility in the correction of fine lines and wrinkles in immunocompetent patients while also offering the added benefit of improving skin texture and skin tightening, with results lasting up to 2 years [ ].
Mazzuco described the use of PLLA to address cutaneous aging of the anterolateral neck in 36 patients, with an average of 1.8 sessions per patient, and an average volume of 3.9 mL injected per patient in each treatment session. The PLLA was diluted in 10 mL of sterile water 2 to 3 days prior to injection and kept refrigerated. Immediately prior to use, the vial was brought to ambient temperature and 0.1 mL of lidocaine 2% was added to each 0.9 mL of reconstituted PLLA. A 1-mL syringe with a 27 G × 4 mm needle was used to inject 0.05 mL of diluted product into the plane between the deep dermis and subcutaneous tissue, with each injection spaced 1 cm apart. Care was taken to manually massage the treated area for 2 minutes postprocedure, and patients were instructed to vigorously massage the neck for 5 minutes, 3 times a day, for 7 days. Only one patient, who reported that she did not follow the posttreatment massage instructions, developed subcutaneous nodules in the anterior neck. The nodules were successfully treated with injection of sterile water, vigorous massage, and intralesional triamcinolone. At the end of the treatment, 91.6% of patients reported they were pleased with their results and stated they would have the procedure done again. All patients were followed for 18 months from the start of treatment, and the improvements in laxity and texture were found to persist throughout this period when judged by 3 independent evaluators [ ].
Hyperdilute Calcium Hydroxylapatite
Calcium hydroxylapatite (CaHA) is a biocompatible, resorbable, injectable soft tissue biostimulator that provides volume replacement and induces extracellular matrix remodeling, improving skin quality, laxity, and rhytids. Commercially known as Radiesse (Merz North America, Raleigh, NC), it is composed of 30% synthetic CaHA microspheres suspended in a 70% aqueous carboxymethyl cellulose gel carrier. When CaHA is hyperdiluted, biostimulation occurs without associated dermal volumization.
Trindade de Almeida investigated the clinical and ultrasonographic improvement induced by 2 sessions of subdermal injection of hyperdiluted (1:4) CaHA in 22 patients with mild or moderate horizontal neck lines and mild or moderate neck laxity. The CaHA was diluted by connecting a 5-mL Luer Lock syringe containing 2 mL of 2% lidocaine to the original 1.5 mL CaHA syringe through a transfer adapter and injecting the 1.5 mL of CaHA into the 5-mL Luer Lock syringe. Then, the Luer Lock 5-mL syringe containing the mixture (1.5 mL CaHA combined with 2 mL of 2% lidocaine) was connected to another Luer Lock 5-mL syringe containing 4 mL of 0.9% saline and at least 20 passes between the 2 syringes were performed to adequately mix the final 7.5 mL total volume. The hyperdilute mixture (1.5 mL CaHA plus 2 mL of 2% lidocaine plus 4 mL of 0.9% saline) was injected using the original 1.5-mL CaHA syringe. The neck was divided into 5 columns, and 1.5 mL of hyperdiluted CaHA was injected into each column by placing 0.1 mL aliquots in retrograde parallel linear threads using a 27G × 0.75-inch needle adapted to the original syringe. In the study, transient pain, ecchymoses, nodule formation (which dissolved with manual massage), a sensation of heat, and a sensation of rough skin were reported by some participants; however, no serious adverse events occurred. Two sessions of subdermal hyperdiluted CaHA injections were well-tolerated and improved horizontal neck lines, neck laxity, and dermal thickness in adult women with mild and moderate cervical aging [ ].
Platysmal banding
Neuromodulators
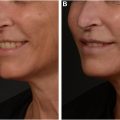
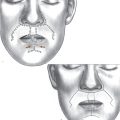
Injection of onabotulinumtoxin A along the mandible and into the platysmal bands relaxes the platysmal muscle, leading to lifting of the neck/lower face and recontouring of the jawline in a technique colloquially known as the “Nefertiti Lift.” [ ] Prior to injection, the platysmal bands may be isolated by having the patient say “eee” or grimace. Subsequently, 2 to 6 intramuscular injections per neckband are placed in a vertical fashion. Finally, 3 to 4 intradermal injections are placed along the inferior aspect of the mandibular border, starting behind the hypothetical point where the nasolabial fold joins the mandible. The suggested dose is 2 to 2.5 U of onabotulinumtoxin A per injection site, for a total of 20 to 30 U per side. Combining hyperdiluted CaHA injections with neuromodulators can lead to significant improvement in neck laxity and platysmal banding ( Figs. 2 and 3 ).