9 Nonandrogenetic Hair Loss
Summary
Keywords: alopecia nonandrogenetic scarring cicatricial nonscarring noncicatricial
Key Points
•Alopecia causes a significant psychosocial burden to society.
•Many scalp disorders other than androgenetic alopecia may lead to hair loss.
•A thorough clinical exam and often laboratory evaluation is necessary to diagnose the cause of hair loss and determine the utility of hair transplantation.
9.1 Introduction
Although androgenetic alopecia is the most common type of hair loss leading to hair transplantation surgery, a variety of scalp disorders may lead to scarring and nonscarring alopecia. A firm knowledge of these disorders is necessary when determining the best course of treatment. This is especially important when treating certain cicatricial/scarring alopecias, as hair transplantation may not be the ideal therapy and may even be deleterious. This chapter reviews the various types of nonandrogenetic alopecia and briefly describes the role of medical and surgical treatment (Video 9.1).
9.2 The Evaluation of Hair Loss
A thorough history and detailed physical exam (PE), in addition to various serum laboratory investigations, will help accurately identify the cause of alopecia for the majority of patients (Box 9.1). A thorough history can aid the clinician in narrowing the potential cause(s) of alopecia. All hair loss patients should be questioned on the timing of their hair loss; gradual hair thinning over a period of years suggests androgenetic hair loss. In women with gradual thinning, it is important to inquire regarding menstruation, acne, and hirsutism to rule out polycystic ovary syndrome (PCOS). Sudden diffuse shedding after an emotional or a physical stressor suggests telogen effluvium (TE) and, less commonly, the diffuse type of alopecia areata (AA). Associated symptoms such as erythema, edema, crusting, pustule, and blister formation are important questions as these changes frequently occur in scarring disorders. In contrast, trichodynia—a complaint of scalp sensitivity or irritation—is nonspecific and may be associated with either scarring or nonscarring alopecia. Scalp burning, pain, and itch may be more commonly associated with various cicatricial alopecias, including lichen planopilaris (LPP), discoid lupus, central centrifugal cicatricial alopecia (CCCA), and dermatomyositis, and neutrophilic cicatricial alopecias including folliculitis decalvans, dissecting cellulitis (DC), and folliculitis keloidalis. Additionally, patients should be asked about general hair care and styling preferences that may contribute to alopecia, including regular use of blow dryers, hair straighteners, and tight braids.
Box 9.1: Evaluation of Hair Loss
A thorough history and detailed physical exam, in addition to various blood laboratory investigations, will help accurately identify the cause of alopecia for the majority of patients.
History: Assess the pattern and extent of hair loss:
•Gradual and progressive hair thinning is consistent with androgenetic alopecia, with or without polycystic ovary syndrome.
•Diffuse rapid shedding is more typical of telogen effluvium and, less commonly, the diffuse form of alopecia areata.
•Rapid, localized patchy hair loss is typical of patch-type alopecia areata.
Physical exam:
•Assess existing hairs:
–Broken hairs, identifiable by their blunt ends, of variable length suggest trichotillomania or traumatic breakage (i.e., regular blow drying, hair straightening, or braiding).
–Peripheral exclamation point hairs suggest alopecia areata.
•Examine the skin in the affected area:
–Frank inflammation suggests an active infectious or scarring disorder.
–Shiny, atrophic skin with follicular ostia dropout suggests a scarring alopecia.
–Nonreflective skin of normal thickness and preserved follicular ostia indicate a nonscarring process.
Trichoscopy: With use of dermatoscopy or videomicroscopy
Aid in the examination of the following: (1) hair shafts, (2) follicular ostia, (3) perifollicular epidermis, and (4) blood vessels.
•Standard microscope or dermatoscope: Hair shaft examination to help identify structural hair abnormalities.
•Videomicroscope (e.g., Folliscope): For determination of hair density (no. of hairs/cm2) and caliber.
Additional diagnostic aides include:
•Skin biopsy: Dermatopathologic evaluation is particularly important for patients whose cause of alopecia is not clear. However, clinical pathologic correlation is often necessary to determine the ultimate diagnosis.
Numerous medications are culprits of telogen, and less commonly anagen, and effluvium (Table 9.1).3 Fortunately, most medication-induced alopecias are nonscarring. However, various chemotherapeutic and biologic drugs have been associated with scarring hair loss.
Table 9.1 Drugs associated with hair loss
•Amphetamines |
•Angiotensin-converting enzyme inhibitors |
•Anticoagulants |
•Anticonvulsants |
•Antidepressants |
•Antifungals |
•Antigout agents |
•Antineoplastics |
•Antipsychotics |
•Antithyroid drugs |
•Beta-blockers |
•Cholesterol-lowering agents |
•Cimetidine |
•Gold-based agents |
•Immunosuppressants |
•Interferon |
•Levodopa |
•Loratadine |
•Nonsteroidal anti-inflammatories |
•Oral contraceptives |
•Propylthiouracil |
•Retinoids |
•Spironolactone |
•Stanozolol |
•Topical minoxidil |
•Topical ophthalmic beta-blockers |
•Vitamin A (over 5,000 IU daily) |
On PE, one should note the distribution and severity of hair loss, which will provide clues to the underlying etiology. For example, localized hair loss is usually seen in AA, whereas diffuse hair loss is more commonly associated with TE, metabolic disorders such as PCOS and the diffuse type of AA. Inspect areas of alopecia for the presence of broken-off, blunted hairs that can be seen in trichotillomania, and “exclamation point” hairs (short hairs whose proximal end is tapered and the distal end is broader) that occur in AA. Scarring is recognized by the absence of follicular ostia. In ambiguous cases, the use of a standard microscope, dermatoscope, or videomicroscope may help distinguish scarring from nonscarring alopecias without the aid of skin biopsies.
A hair pull test will aid in the assessment of current hair shedding. It is important to ask the patient if their hair was washed on the day of clinical evaluation as freshly washed hair often results in a falsely negative hair pull exam. The ability to pull more than five or six hairs when grasping approximately 60 hairs denotes a positive hair pull test. The hair tug test is an additional clinical examination that helps identify hair fiber fragility. The mid hair shaft is held with one hand and the distal hair shaft with the other, pulling away from the scalp with the distally placed hand. A positive hair tug test is a sign of hair breakage.1,2
Serum laboratory examinations are often helpful unmask potential triggers of nonscarring alopecia. A thorough history and PE can help guide the clinician when choosing the appropriate serum tests. Testing for iron, zinc, and vitamin D deficiencies may be most beneficial for TE patients. Thyroid function tests and thyroid antibodies are useful for both AA and TE patients as thyroid dysfunction, autoimmune related or not, may be seen with these types of hair loss. Free and total testosterone and DHEAS (dehydroepiandrosterone sulfate) are important exams when evaluating for PCOS or other disorders of androgen excess such as an androgen-secreting neoplasm. Antinuclear antibody by indirect fluorescent antibody (to evaluate both the titer and pattern) and complement levels are necessary when a connective tissue disease such as lupus erythematosus is suspected (Table 9.2).
Table 9.2 Select laboratory tests in the investigation of hair loss
Disease | Laboratory examinations |
Thyroid disease | TSH |
Vitamin and mineral deficiencies | Serum ferritin, zinc, vitamin D |
Polycystic ovary syndrome | Serum free and total testosterone, DHEAS, SHBG, prolactin |
Lupus erythematosus | Antinuclear antibody by IFA, complements (C3, C4, CH50), CBC (anemia and leukopenia) |
Abbreviations: CBC, complete blood cell count; DHEAS, dehydroepiandrosterone sulfate; ESR, erythrocytes sedimentation rate; SHBG, sex-hormone–binding globulin; TSH, thyroid-stimulating hormone. | |
Though user dependent, dermoscopy of the scalp and hair, termed “trichoscopy,” is a noninvasive, rapid technique to aid in the diagnosis of various alopecias. Multiple structures may be visualized using trichoscopy, including hair shafts, follicular ostia, perifollicular epidermis, and blood vessels (Table 9.3).
Table 9.3 Trichoscopy: Structures and patterns
Disease | Trichoscopic findings | Anatomic correlate |
Alopecia areata | •Exclamation point hairs •Yellow dots (regularly distributed) | •Proximally tapered hair shaft •Follicular ostia filled with keratotic material and/or sebum |
Androgenetic alopecia | •Hair shaft thickness heterogeneity •Vellus hairs •Oily-appearing yellow dots | •Lightly pigmented hairs, <3 mm in length and <30 µm thick •Follicular ostia filled with sebum > keratotic material |
Trichotillomania | Flame hairsa | Hair residue from pulling anagen hairs, correspond to distorted hair shafts on pathology |
Tinea capitis | Corkscrew, comma hairs | Likely a result of subsequent cracking and bending of the hair shaft filled with hyphae |
LPP | •White dots •Perifollicular scaling •Elongated vessels | •Empty follicular ostia and eccrine sweat gland ducts •Formation of tubular scaly structures around hair shafts |
FFA | Grey dots | •Due to loose melanin, fine melanin particles or melanin “dust” in melanophages or free in the deep, papillary, or reticular dermis •Widened infundibula filled with keratotic material |
Discoid lupus | •Dark yellow dots •Red dots •Thick arborizing vessels | Widened infundibula plugged by keratin and surrounded by dilated vessels and extravasated erythrocytes |
Abbreviations: CCCA, central centrifugal cicatricial alopecia; LPP, lichen planopilaris; FFA, frontal fibrosing alopecia. a Flame hairs are not specific to trichotillomania. They may also be seen in alopecia areata, traction alopecia, CCCA, and acute chemotherapy- and radiotherapy-induced alopecias. | ||
In the presence of a scarring alopecia, accurate diagnosis is usually established by obtaining a 4-mm punch biopsy at the advancing inflammatory border. Scarred regions should be avoided when selecting the biopsy location, as these areas are likely to show nonspecific changes. The biopsy should be performed in the direction of hair growth and penetrate into subcutaneous fat, yielding the optimal specimen for both vertical and horizontal sectioning. Vertical sectioning is important for examining features such as inflammatory infiltrates, scarring, and the presence of infectious organisms. Horizontal sectioning is important for determining the ratio of hair follicle stages (anagen vs. telogen) in addition to the presence of follicular miniaturization (terminal vs. vellus hairs).
9.3 Causes and Treatment of Hair Loss
The categories of hair loss are broadly classified as either cicatricial or noncicatricial. Cicatricial alopecia is caused by a heterogeneous group of conditions, most of which have scarring and atrophy as a common end point (Table 9.4 and Table 9.5). Clinically, this scarring is recognized by the absence of follicular ostia on shiny, atrophic skin. In contrast, noncicatricial alopecias demonstrate follicular ostia preservation on skin with normal reflectivity and thickness (Box 9.2, Table 9.6 and Table 9.7).
Table 9.4 Common causes of cicatricial alopecia
Infection: •Tinea capitis/kerion |
Inflammatory diseases: |
•Central centrifugal cicatricial alopecia •Folliculitis keloidalis •Dissecting cellulitis •Lichen planopilaris •Frontal fibrosing alopecia •Discoid lupus erythematosus |
Traumatic causes: •Injurya •Radiation •Postoperative scarring |
Neoplastic processes: •Basal cell carcinoma •Squamous cell carcinoma |
a Injury, including iatrogenic, is often a preceding event to erosive pustular dermatosis of the scalp. |
Table 9.5 Uncommon causes of cicatricial alopecia11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28
Infection: |
•Varicella |
Inflammatory diseases: •Sarcoidosis •Erosive pustular dermatosis of the scalp •Mastocytosis •Bullous lichen sclerosus •Necrobiosis lipoidica •Cicatricial pemphigoid •En coup de sabre morphea •Acne necrotica/folliculitis •Chronic graft versus host disease |
Traumatic causes: •Alopecia associated with birth injury—caput succedaneum |
Neoplastic: •Visceral malignancy metastasis •Leukemia cutis •Extramammary Paget disease •Angiosarcoma •Desmoplastic melanoma |
Genetic causes: •Aplasia cutis congenital •Incontinentia pigmenti •Porphyria cutanea tarda •Ulerythema ophryogenes •Marie-Unna hereditary hypotrichosis |
Medications: •Epidermal growth factor receptor inhibitors (cetuximab, panitumumab) •Human epidermal receptor tyrosine kinase inhibitors (erlotinib, gefitinib) |
Table 9.6 Common causes of noncicatricial alopecia
Metabolic abnormalities |
Vitamin and mineral deficiencies (iron, vitamin D, and zinc) |
Thyroid disease: •Polycystic ovary syndrome |
Effluviums: •Telogen effluvium •Anagen effluvium |
Autoimmune disorders: •Alopecia areata |
Traumatic causes: •Trichotillomania •Traction alopecia •Pressure-induced alopecia |
Hair shaft abnormalities (with increased hair fragility) |
Genetic: •Trichorrhexis nodosa •Monilethrix •Pili torti •Trichorrhexis invaginata •Trichothiodystrophy |
Acquired: •Bubble hair |
Congenital: |
Table 9.7 Uncommon causes of noncicatricial alopecia29–,33
Infection: •Syphilis |
Inflammatory diseases: •Lupus panniculitis |
Neoplastic processes: •Alopecia mucinosaa •Syringolymphoid hyperplasiaa |
Genetic/congenital disorders: •Ectodermal dysplasias •Lipedematous alopecia •Loose anagen syndrome |
Other: •Hair-cutter ant attack (Pheidole ants, endemic to Iran) |
a Mycosis fungoides or Sezary syndrome may precede, coincide, or follow the diagnosis of alopecia mucinosa. Therefore, these patients must be followed up closely. |
Box 9.2: Cicatricial Alopecia
Early identification of active scarring will facilitate diagnosis and improve clinical outcome.
Due to risk of disease reactivation, only select cases of idiopathic scarring alopecia should be considered for surgical correction. Current active inflammation is a contraindication to surgery.
Great caution and long-term follow-up are needed when transplanting into areas of scarring secondary to previous malignancy as the patient and clinicians may have difficulty recognizing early recurrence.
Key Points: Nonscarring Alopecia
•Nonscarring alopecia is commonly caused by metabolic abnormalities, drug-induced effluviums, autoimmune disease, and traumatic disorders.
•Dermatoscopic examination and laboratory evaluation are helpful in the diagnosis of various nonscarring alopecias.
•Various types of nonscarring alopecia may ultimately require hair transplantation, including polycystic ovary syndrome, telogen effluvium, especially with underlying androgenetic alopecia, and triangular alopecia.
9.3.1 Nonscarring
Metabolic Abnormalities
Vitamin and Mineral Deficiencies
Zinc deficiency:
In a mouse model, high doses of oral zinc have been shown to inhibit hair growth; yet, the same treatment can delay (but not prevent) the onset of chemotherapy-induced alopecia.9 Conditions such as acrodermatitis enteropathica, which results in severe zinc deficiency and is characterized by alopecia among other symptoms, are proof that zinc plays an important role for hair. In a recent study by Cheung et al, zinc deficiency was present in only 9.6% of their study population.9 Therefore, the clinician should consider zinc supplementation only if a deficiency exists. See Table 9.8 for zinc dosing suggestions.
Table 9.8 Laboratory evaluation and supplementation suggestions for hair loss (TE) patients with vitamin and mineral deficiencies
Vitamin/mineral | Screening lab | Deficiency level | Daily Supplementation |
Zinc Iron Vitamin D | Plasma zinc level Serum ferritin Serum 25-hydroxyvitamin D | <60 μg/dL <40 ng/mL <30 nmol/L | Zinc gluconate 100 mg or zinc sulfate 110 mg × 3 mo (then recheck level) Oral ferrous sulfate 325 mg or ferrous gluconate 324 mg × 3 mo (then recheck level) 25-Hydroxyvitamin-D < 20 nmol/L: 50,000 IU of vitamin D3 weekly × 6–8 wk, then 1,000 IU daily thereaftera 25-Hydroxyvitamin-D 20–30 nmol/L: OTC vitamin D supplements (D2 or D3) at 600–800 IU dailya |
Abbreviations: OTC, over the counter; TE, telogen effluvium. a Serum 25-hydroxyvitamin D levels are reevaluated once every 3 months until no longer deficient, then daily OTC supplements are continued. Source: Adapted from Kantor et al.10 | |||
Iron deficiency: Some authors believe iron deficiency may be related to multiple nonscarring alopecias, including TE as well as AA and androgenetic alopecia. While causality has not been established, nor has iron supplementation been proven to impact hair growth,10,11 many hair experts treat iron deficiency in the absence of anemia. When investigating iron deficiency with or without anemia, it is important to order a complete blood count (CBC) and ferritin as well as an iron panel as ferritin is an acute-phase reactant and may be elevated in the setting of infection, inflammation, or malignancy. It is important to investigate the underlying cause of iron-deficiency anemia, especially in the older patient population as gastrointestinal blood loss is an important cause of iron-deficiency anemia.
Thyroid Disease
Thyroid disease should also be considered in the evaluation of women with diffuse thinning and TE. Although data regarding the effect of thyroxine supplementation on TE is lacking, thyroid hormone has been proven to prolong the anagen phase.12 Given diffuse scalp involvement, the donor area may also be compromised, making hair transplantation difficult.
Polycystic Ovary Syndrome
Polycystic ovary syndrome is a disorder resulting in metabolic and reproductive abnormalities and affects up to 8% of women of child-bearing potential. It is characterized by the triad of (1) ultrasound evidence of polycystic ovaries, (2) chronic anovulation, and (3) hyperandrogenism. Additionally, other causes of hyperandrogenism and anovulation (i.e., androgen-secreting tumors, Cushing syndrome, and congenital adrenal hyperplasia) must be ruled out. Women with PCOS typically have irregular menses and increased androgen levels which lead to acne, hirsutism, and potentially androgenetic alopecia. In addition to decreasing the percentage of anagen hairs, androgens stimulate the conversion of scalp terminal hair follicles to vellus hair. An initial laboratory evaluation should include serum total and free testosterone, SHBG (sex hormone–binding globulin), DHEAS, prolactin, and a pelvic/transvaginal ultrasound. Female pattern androgenetic alopecia is the most common pattern of hair loss among women with PCOS and although less common, hair loss in a male pattern is also possible. Medical therapy such as spironolactone, finasteride, or cyproterone acetate, which either block androgen receptor binding or may inhibit 5-α-reductase activity, may result in improvement of alopecia after 6 to 12 months of therapy. If results are still unsatisfactory, hair transplantation to cosmetically significant regions may be helpful.13,14
Effluviums
Telogen Effluvium
Telogen effluvium is one of the most common types of alopecia among presenting hair patients. Fortunately, it is a nonscarring alopecia and although it typically resolves by 6 months, chronic TE lasting over 6 months also occurs. Patients present with diffuse hair loss (usually <50% of scalp hair is shed) that typically begins around 3 months after a triggering event. The central part may be widened, with bitemporal thinning as well. Unlike androgenetic alopecia, TE is characterized by a positive hair pull test.
Often very alarmed by the excess hair shedding, patients may bring plastic bags of their shed hair (“hair bag sign”). The timing and causes of hair loss may differ depending on the type of TE. There are six types of TE: (1) immediate anagen release, (2) delayed anagen release, (3) immediate telogen release, (4) delayed telogen release, (5) short anagen phase, and (6) chronic TE (see Table 9.9).
Table 9.9 Telogen effluvium (TE)
Type of TE | Triggers | Timing of initial hair shedding |
Immediate anagen release | Fever | Days |
Delayed telogen release | Postpartum | ~2–3 mo after delivery |
Immediate telogen release | Topical minoxidil | 2–8 wk after treatment initiation |
Delayed telogen release | Seasonal hair shedding | Within weeks of seasonal change (typically winter to spring) |
Short anagen phase | Genetica | N/A: inability to grow long hair |
Chronic TE | Often not found | mo, lasts > 6 mo to several years |
a Short anagen phase occurs in hereditary hypotrichosis, ectodermal dysplasia, and in otherwise healthy children. | ||
As TE has numerous potential triggers, including medications, physiologic stressors, as well as nutritional, endocrinologic, and autoimmune disorders, a complete history and PE in addition to serum evaluation (see Table 9.10) are necessary to elucidate an underlying cause.
Table 9.10 Laboratory evaluation for patients with telogen effluvium
Disease | Laboratory examinations |
Thyroid disease | TSH, free T4, thyroid antibodies |
Vitamin and mineral deficiencies | Serum ferritin and iron panel, zinc, vitamin D |
Anemia (iron deficiency) | CBC with differential |
Connective tissue diseasea | Antinuclear antibody by IFA, complements (C3, C4, CH50) |
Abbreviations: DHEAS, dehydroepiandrosterone sulfate; IFA, indirect fluorescent antibody; SHBG, sex-hormone–binding globulin; TSH, thyroid-stimulating hormone. a These laboratory evaluations should be ordered only if, after a through history and PE, the clinician suspects connective tissue disease. | |
TE may unmask an underlying androgenetic alopecia, in which case hair loss can be progressive. Counseling is a vital component of therapy for TE patients. In the majority of cases, the natural history of TE includes 3 to 6 months of shedding before cessation and regrowth is noted at 3 to 6 months after trigger removal. However, significant regrowth may take 12 to 18 months. In addition to trigger removal, minoxidil is often employed given its effect on prolonging the anagen phase. Hair transplantation ideally should not be performed prior to resolution, as it is difficult to properly identify the regions of greatest cosmetic significance and areas of the donor with dormant follicles may be discarded as alopecic tissue. Hair transplantation may be necessary after the TE episode has resolved, especially in those with underlying androgenetic alopecia not responding to medical therapy.15
Anagen Effluvium
The anagen growth phase of hair is characterized by mitotic and metabolic activity. Any event, most often chemotherapy or radiotherapy to the head and neck, may cause the abrupt cessation or impairment of mitotic or metabolic hair follicle activity and subsequent proximal hair shaft weakening and breakage (either within the hair canal or complete failure of hair shaft formation). Given their effect against DNA replication, the most common chemotherapeutics to cause anagen effluvium include (1) antimetabolites, (2) alkylating agents, and (3) mitotic inhibitors. Less often, nutritional deficiency, immunobullous disease, AA, connective tissue disease, secondary syphilis, and toxin/medication exposures may cause anagen effluvium (see Table 9.11).
Table 9.11 Causes of anagen effluvium
Agent | Class | MOA | |
Most common | |||
Chemotherapeutics | |||
5-Fluorouracil | Antimetabolites | Thymidylate synthetase inhibition | |
Cyclophosphamidea | Alkylators | DNA replication inhibition | |
Paclitaxel | Mitotic inhibitors | Tubulin inhibitor | |
Doxorubicin | Cytotoxic Abx | Topoisomerase inhibition | |
Less common | |||
Other medications | Bismuth, levodopa, colchicine, busulfan,a EGFR inhibitors,a and cyclosporine | ||
Nutritional | Severe protein energy malnutrition | ||
Immunobullous dz | Pemphigus vulgaris | ||
Primary hair disorders | Alopecia areata | ||
Toxin exposures | Mercury, boron, thallium | ||
Connective tissue dz | Systemic lupus erythematosus | ||
Infection | Secondary syphilis | ||
Other | Bone marrow transplantationa | ||
Abbreviations: dz, disease; Abx, antibiotic; EGFR, epidermal growth factor receptor; MOA, mechanism of action. a These therapies may result in permanent hair loss.18 | |||
Anagen effluvium is typically completely reversible, as the insult is only on the proliferating cells and the bulge stem cells (which are quiescent) are able to reinitiate follicle growth. Hair regrowth is apparent within 1 to 3 months of removal of the insult. Patients have a higher risk of permanent hair loss in the setting of bone marrow transplantation, Busulfan, and epidermal growth factor receptor inhibitor therapy and may ultimately require hair transplantation (assuming adequate donor hair is present).16
Loose Anagen Hair Syndrome
Loose anagen hair syndrome (LAHS) is a female-predominant genetic disorder likely resulting from premature and abnormal keratinization of the hair inner root sheath. This results in loose anagen hair which is easily and painlessly pulled from the scalp. LAHS primary affects light-haired children and less commonly adults. The scalp hair is typically short and dull and irregular alopecic patches occur as a result of easily plucked anagen hairs. On microscopic hair shaft examination, the loose anagen hair (which should comprise >50% of hairs on trichogram) lacks a sheath and has a characteristic “wrinkled sock” appearance. Most patients do not require surgical intervention as LAHS typically resolves spontaneously by adolescence or adulthood.
Autoimmune Disorders
Alopecia Areata
One of the most common hair disorders encountered in dermatology, AA, is an autoimmune, nonscarring form of hair loss. It typically presents with well-demarcated, coin-sized patches of noncicatricial alopecia scattered on an otherwise normal-appearing scalp, or in other hair-bearing regions (Fig. 9.1). Rarely, it presents with a large band-like patch of alopecia extending from bilateral temporal scalp to the occipital scalp (ophiasis pattern; Fig. 9.2), or with hair loss over the frontal and crown regions (sisaipho pattern). The diffuse form of alopecia may mimic TE; however, it is easily distinguished by the abrupt depigmentation of scalp hair, termed the “white overnight” phenomenon. In severe cases, hair loss affects the entire scalp (alopecia totalis), or the entire body (alopecia universalis).17,18,19
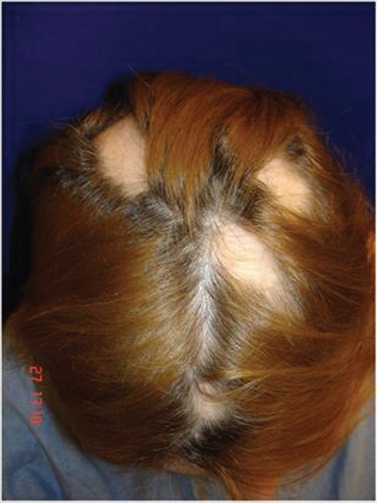
Fig. 9.1 Patch-type alopecia areata with several, well-demarcated alopecic patches on the scalp.
Related posts:
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
 Transplanting into Areas of Cicatricial Alopecia
Transplanting into Areas of Cicatricial Alopecia
 Special Considerations for Postoperative Care in Follicular Unit Excision
Special Considerations for Postoperative Care in Follicular Unit Excision
 Hairline and Recipient Area Repair of Poor Previous Transplantation
Hairline and Recipient Area Repair of Poor Previous Transplantation
 Ergonomics in Hair Restoration Surgery: FUE Technique
Ergonomics in Hair Restoration Surgery: FUE Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


