Metacarpal fractures are among the most common fractures of the upper extremity. Surgical management is generally offered for unstable or significantly displaced fractures. A more conservative, nonsurgical approach, however, may provide safe, rapid recovery while maintaining normal active range of motion. This article reviews the nonsurgical approach, protocols, and outcomes of metacarpal fractures.
Key points
- •
Metacarpal fractures are among the most common fractures of the upper extremity.
- •
Surgical management is generally offered for unstable or significantly displaced fractures.
- •
A more conservative, nonsurgical approach, however, may provide safe, rapid recovery while maintaining normal active range of motion.
Introduction
Fractures of the metacarpus or phalanx are common, accounting for 40% of upper extremity fractures. Treatment of these common fractures varies widely, often depending on surgeon preference and experience. Other factors that play a role in treatment include hand dominance, age, comorbidities, occupation, compliance, fracture anatomy, and mechanism of injury.
Developing individualized treatment plans for these fractures can be challenging. Availability of peer-reviewed publications related to patient outcomes is limited. As no definitive agreement on the best practice for treatment exists, patients with similar fracture patterns, mechanism of injury, and patient characteristics may be treated with either nonoperative management (no or closed reduction with or without splint immobilization) or operative treatment (closed or open reduction with internal fixation). Each of these options has advantages and disadvantages, and the best method of treatment remains controversial. Review of the current literature highlights the need to provide surgeons with outcomes-based evidence regarding the treatment of hand fractures.
Basic treatment strategies are designed to restore function to the hand. Most nondisplaced fractures of the metacarpal are typically allowed to heal with simple immobilization for a period of 3 to 4 weeks. Patients can then resume normal range of motion with or without the need of therapy. Ultimately, then the goal of fracture management is to restore function, normal range of motion, and anatomy with a pain-free grip. Many metacarpal fractures, however, are displaced and traditionally have required surgery to restore normal anatomic alignment. Nonsurgical approaches, however, may offer benefits to the care of patients with metacarpal fractures.
Before embarking upon any type of treatment for metacarpal fractures, the surgeon should identify the goals of the treatment ( Box 1 ). Many authors have required other goals, including anatomic alignment and maintenance of length of the metacarpal to try to prevent secondary deformities. These goals, however, are not as important if normal function has been preserved despite the characteristics of the fracture. For example, many patients need radiographs for a given new problem. Incidental findings of conditions such as severe degenerative joint disease or old fractures, are often noted but not treated, because the patient is not symptomatic in these areas. If the radiograph was not done, the patient and surgeon would not have known of these incidental findings. The same is true for metacarpal fractures. If a patient is examined before the radiograph is viewed and found to have normal range of motion with no scissoring, what would be gained by operating on the hand even though the radiograph show them to be displaced or involving multiple metacarpals? The patient already has normal range of motion, making it difficult for surgery to improve the outcome. In fact, the opposite is true; surgery could only diminish the hand function through mechanisms described previously or at best maintain status quo. If this last statement is true, there would be a very limited indication to operate on patients with normal range of motion with displaced or multiple metacarpal fractures. It should be noted that treatment strategies may be different for intra-articular fractures, since anatomic alignment and the need for open reduction in this scenario are more critical to try to prevent subsequent degenerative arthritic changes within the joint.
Maintain normal range of motion
Restore normal range of motion
Restore grip strength
No residual pain
Normal digital alignment
Minimize stiffness
Bone union
Restore normal functional capacity
An important part of a conservative management of patients with metacarpal fractures at the authors’ institution is the immediate start of home therapy. A night splint can be given to protect the fracture and decrease pain at nighttime, but during the day, the patient maintains his or her full active range of motion with flexion and extension exercises. Formal hand therapy is usually not required. Patients do not have a period of immobilization except for the period of time from the injury to the time they see the surgeon. Follow-up office visits at 1 week and then 3 weeks are needed to make sure the patient has not developed scissoring or other negative sequelae. The patient is limited from hard labor but allowed to use the hand, with pain being the guiding factor of whether to limit movement.
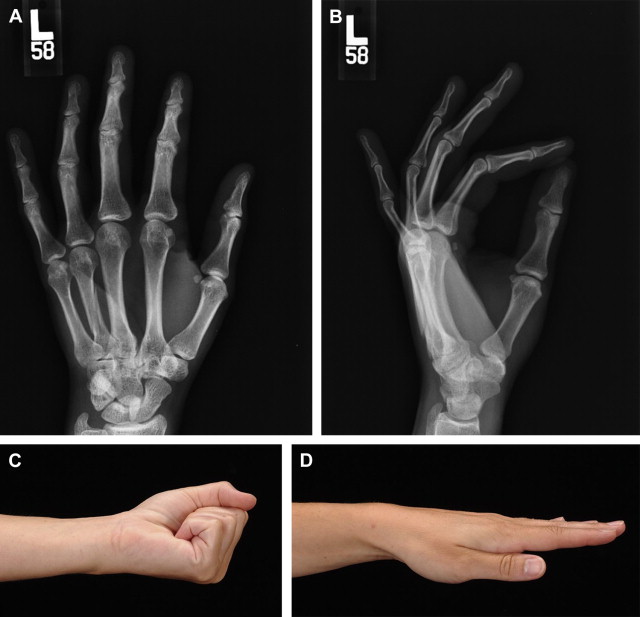
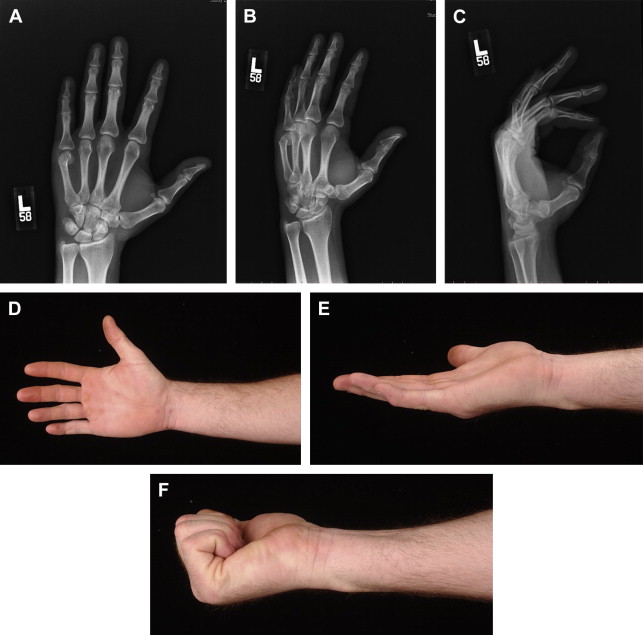
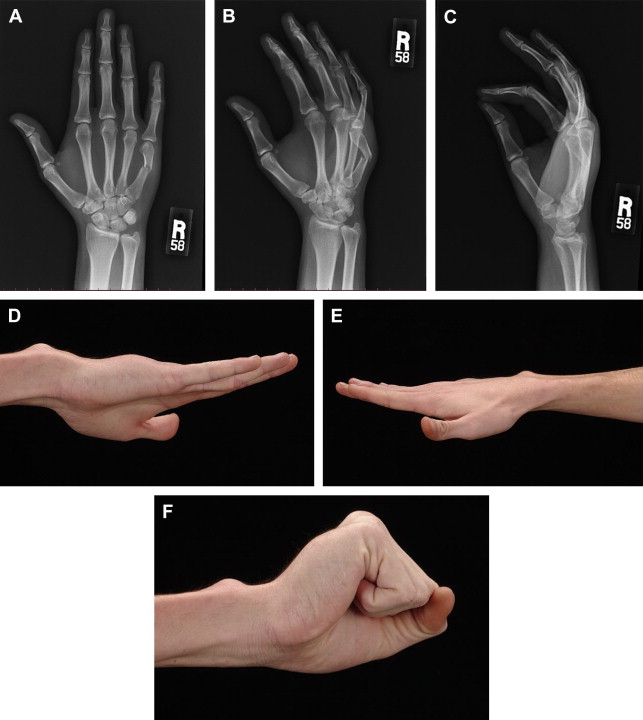
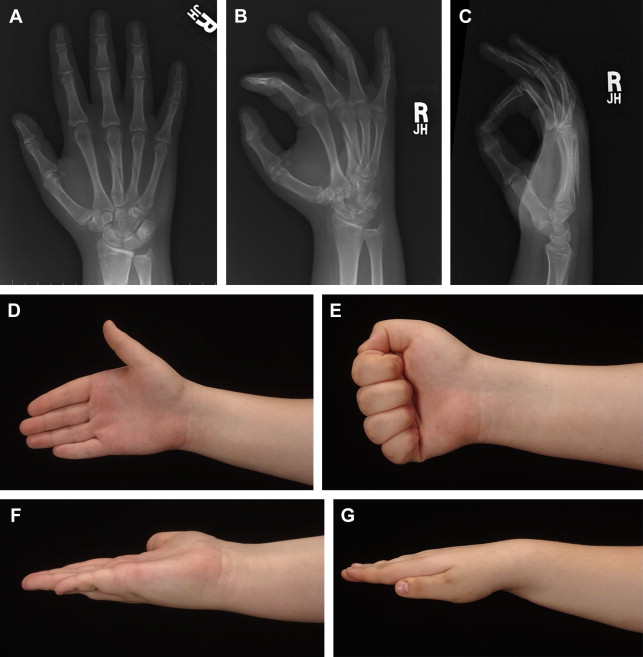
Fig. 1 illustrates a patient that sustained a third metalcarpal spiral fracture that had minimal displacement. The patient wanted surgery, believing it would restore normal function faster. The postreduction with rigid lag screw fixation revealed normal anatomic alignment. The postoperative course, however, was complicated with stiffness that necessitated formal physical therapy. Normal motion was finally obtained but somewhat prolonged (see Fig. 1 ). Similar fractures can be treated conservatively with rapid return to full activities ( Fig. 2 ). Metacarpal neck fractures tolerate conservative management extremely well ( Fig. 3 ). Even metacarpal shaft fractures can be treated in a conservative fashion despite significant dorsal angulation ( Fig. 4 ). These patients must initiate aggressive early motion to maintain normal function. The dorsal hump is usually cosmetic and does not foster physical limitations. Occasionally a palmar prominent metacarpal head can cause tenderness on gripping objects, but this is also uncommon. Multiple metacarpal fractures can also be treated nonoperatively with early active motion ( Fig. 5 ). The key to success is demonstrating normal motion with no scissoring or malalignment and regular follow-up visits. What defines stability of a fracture is an interesting concept. Fractures can be significantly displaced and considered unstable yet still heal with normal function with a conservative approach ( Fig. 6 ). Clinical studies defining the extent of the displacement that will compromise healing or function still need to be done.