21
Neutrophilic Dermatoses
This group of disorders, in an untreated state, is characterized by infiltrates of neutrophils within the skin. In addition, these dermatoses lack an identifiable infectious etiology, despite the presence of neutrophils (Fig. 21.1). There can be significant overlap in the clinical presentations of the neutrophilic dermatoses; for example, in a patient with acute myelogenous leukemia, bullous pyoderma gangrenosum may be difficult to distinguish from Sweet’s syndrome. In addition, infiltrates of neutrophils can occur in other organs, particularly the joints, eyes, lungs, and bones. Bone involvement raises the possibility of SAPHO (synovitis, acne, pustulosis, hyperostosis, osteitis) syndrome.
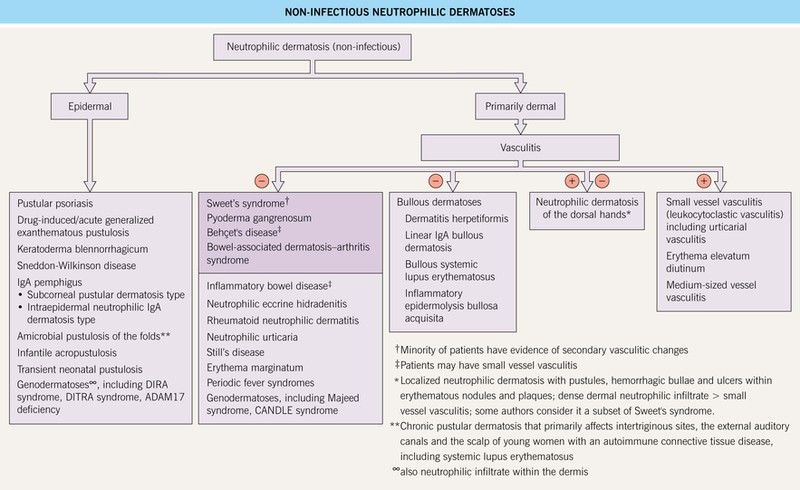
Fig. 21.1 Non-infectious neutrophilic dermatoses. Entities in the darker box are discussed in this chapter. CANDLE, chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature; DIRA, deficiency of interleukin-1 receptor antagonist; DITRA, deficiency of the IL-36R antagonist.
Sweet’s Syndrome (Acute Febrile Neutrophilic Dermatosis)
• Acute onset of erythematous edematous papules and plaques that are tender, but not pruritic; if the edema is intense, the lesions may become bullous and, occasionally, they resemble erysipelas; favored sites are the face, neck, upper trunk, and upper extremities (Fig. 21.2).




Fig. 21.2 Spectrum of cutaneous findings in Sweet’s syndrome. A Edematous erythematous papules and plaques on the neck of a patient with acute myelogenous leukemia. B Markedly edematous plaques on the upper back, some of which are pseudovesicular while others are becoming bullous. C Some of the edematous lesions have a targetoid appearance. D Central hemorrhagic crusts within facial plaques. B, D, Courtesy, Kalman Watsky, MD; C, Courtesy, Mark Davis, MD.
• Less commonly, nodules develop due to neutrophilic panniculitis or pustules form within the plaques; a variant occurs on the dorsal aspect of the hands and is referred to as ‘neutrophilic dermatosis of the dorsal hands’ (Fig. 21.3).

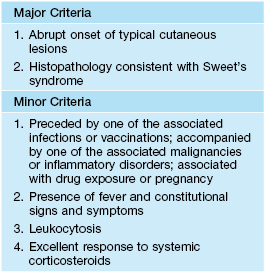
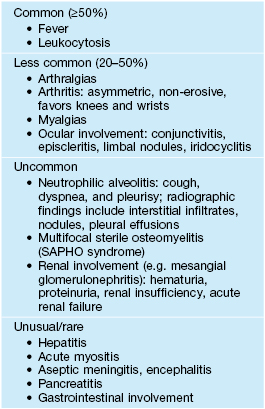
• Associated systemic findings include fever, malaise, and arthralgias, and a peripheral leukocytosis is commonly observed (Table 21.1); some patients also develop systemic manifestations, including ocular, pulmonary, and skeletal involvement (Fig. 21.4, Table 21.2).

• DDx: bullous pyoderma gangrenosum, neutrophilic eccrine hidradenitis, erysipelas, erythema multiforme, causes of pseudocellulitis (see Table 61.2), infectious cellulitis, vasculitis (urticarial, small vessel, septic), halogenoderma, periodic fever syndromes, as well as additional entities in Fig. 21.1.
• Rx:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


