44. Necklift
Sumeet Sorel Teotia, Foad Nahai
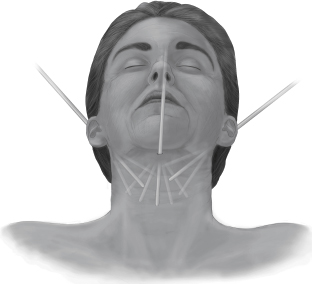
VISUAL CRITERIA FOR A YOUTHFUL NECK 1 (Fig. 44-1)
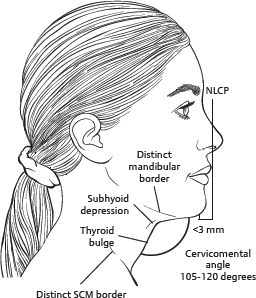
Fig. 44-1 Visual criteria for a youthful neck. (NLCP, Nose-lip-chin plane; SCM, sternocleidomastoid.)
■ A distinct inferior mandibular border
■ A visible subhyoid depression
■ A visible thyroid cartilage bulge
■ A visible anterior border of the sternocleidomastoid muscle
■ A cervicomental angle of 105-120 degrees
SENIOR AUTHOR TIP: Neck recontouring is an integral part of necklifting and often is all that is required.
■ Thus, a corollary to a youthful neck comprises the visual criteria for an aging neck.
VISUAL CRITERIA FOR AN AGING NECK2
■ An obtuse cervicomental angle, caused by:
• Loose, excess skin
• Excess subplatysmal fat
• Excess preplatysmal fat
• Low position of hyoid bone
■ Cervical spinal compression changes related to age
■ An aging chin
■ An aging lower face
■ Effacement of a sharp mandibular border
SENIOR AUTHOR TIP: In addition to thinking of the neck as youthful or aged, we must also consider its shape or contour. Some patients have a full neck with little contour despite normal skin elasticity with no excess skin. These are ideal candidates for recontouring only, with no skin alterations.
PREOPERATIVE EVALUATION3
Evaluating individual components of an aging neck guides toward an appropriate surgical algorithm.
SKIN
■ Skin quality, with rhytids at rest and during animation, is evaluated in detail.
SENIOR AUTHOR TIP: I also look for the deep or etched transverse neck lines.
■ Apparent excess skin
• Redrapes after recontouring with no excision of skin usually necessary
• Requires adequate elasticity to redrape
• Local fat removal and platysmal plication often adequate
■ Real excess skin
• Extends below the thyroid cartilage
• Extends posteriorly beyond sternocleidomastoid muscle
• Excision of skin is necessary.
• A retroauricular skin incision is necessary.
• A submental skin incision is usually necessary.
■ Evaluating skin excess helps to determine the final direction of skin flap redraping.
■ Hairline distortions can be prevented by adequate skin evaluation.
■ Skin quality is inversely related to the length of the incision required.
TIP: Adequate skin elasticity is essential for short-scar procedures. Skin damage and actinic changes require a full-length retroauricular incision because of the increased need to redrape.
FAT
■ The difference between subcutaneous (preplatysmal) and deep (subplatysmal) fat is evaluated. (Fig. 44-2)
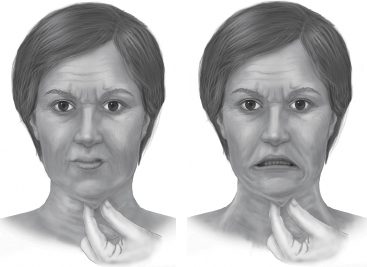
Fig. 44-2 Subcutaneous and deep fat is evaluated.
• Submental fat can be pinched in the submental area at rest.
• Preplatysmal and subplatysmal fat can be discerned by pinching the submental area during contraction.
■ Fat removal has the most dramatic contouring effect.
PLATYSMA4
■ Static (passive) or dynamic (active) platysmal banding is evaluated.
SENIOR AUTHOR TIP: I look for and make a note of the central and lateral platysmal bands.
■ Imperfections in the neck and jaw shadows are noted.
■ Skin excess often accompanies platysmal banding.
■ The neck and face interface is assessed, because platysma decussates above the youthful jawline.
■ The location, direction, and distance between platsymal bands are noted.
■ Pathogenesis of platysmal banding is controversial.5–7
• A contracted platysma creates a hammock between the jawline and clavicle.
• The contraction of muscle fibers creates a bow-string effect away from the tubular neck.
• The bow-string effect is countered by superficial cervical fascia.
• Age-related changes to the fascia allow contents of platysma (fat and other structures) to “bulge,” creating bands (Fig. 44-3).
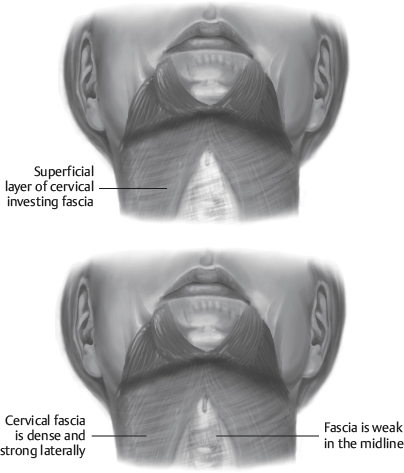
Fig. 44-3 Platysmal banding.
DIGASTRIC MUSCLES8
■ In a fatty neck, digastric muscles are not easily evaluated.
■ In a thin neck, they can bulge below the inferior border of the mandible, creating a subtle but important irregular contour.
■ A persistent bulge after submental fat excision can be caused by prominence of the digastric muscles.
■ The status of digastric muscles is best evaluated intraoperatively, after removal of subcutaneous fat.
SUBMANDIBULAR GLAND9
■ Prominence of the gland below the mandibular rim within the submandibular triangle is evaluated.
■ In a fatty neck, this is often not possible.
■ Intraoperative evaluation is necessary in most cases.
■ Flexing a patient’s neck may help to accentuate a locally bulging deformity from the gland.
MANDIBULOCUTANEOUS LIGAMENT
■ Jowls may result from tethering of the relaxing facial tissues at this ligament.
■ The volume of jowling is evaluated with the patient in a supine position.
■ Lower facial aging transmits its effects on the upper neck, and mandibular angle effacement is important to note posteriorly, along with inferior displacement of jowls.
CHIN
■ The chin should be evaluated in reference to facial proportions.
■ Occlusion and the angle classification are noted.
■ Demineralization of the lower jaw and teeth from age or pathological causes can influence the chin and overlying soft tissues, creating a shortened submental space and influencing anterior neck contour.
■ Hypogenia or microgenia affects the ideal neck contour.
■ An alloplastic chin implant or an osseous genioplasty may complement anterior neck contour.
SENIOR AUTHOR TIP: Look for the submental crease and assess chin ptosis (witch’s chin).
INFORMED CONSENT
Before initiating treatment, the goals, inherent risks, and benefits of a particular treatment are discussed with the patient. An intervention is chosen only after an honest conversation with the patient to define goals and expectations that can readily and safely be met. A thorough knowledge of anatomy of the neck will help to prevent complications (see Chapter 30).
OPTIONS FOR NECK REJUVENATION
Developing an algorithm based on anatomy and clinical evaluation will help to improve neck contour. A logical, “layered” approach can help to plan steps in an operation and address each component of the neck.
■ Superficial tissues
• Skin
• Subcutaneous fat
■ Intermediate tissues: Platysmal muscle and banding
■ Deeper tissues
• Anterior belly of digastric muscles
• Submandibular gland
• Suprahyoid fascia
• Subplatysmal fat pad
NONSURGICAL OPTIONS FOR NECK REJUVENATION
The role for injectable materials such as hyaluronic acid fillers and fat injections is not defined, particularly in primary neck rejuvenation. It may be reserved for secondary corrections.
SENIOR AUTHOR TIP: Currently, injectables have a limited role as do nonsurgical skin-tightening technologies.
BOTULINUM TOXIN
■ Use of botulinum toxin has been suggested.10–12
■ May delay eventual surgical procedure
■ May be useful supplement to surgery and for postsurgical defects of persistent banding
■ Platysmal bands are injected with botulinum toxin.
■ Technique involves grasping bands and distracting them away from the neck.
■ Usual starting dose is 10-30 units in women, 10-40 units in men and women receive 2-12 injections per band and men receive 3-12 injections.
■ A total of approximately 40-100 units is used (Botox).
SENIOR AUTHOR TIP: The relatively large number of units required makes treatment with toxins very expensive, especially in the long term.
■ Best results in younger patients with active (rather than passive) bands
■ Not to be used where significant excess skin is present
■ Not to be used in older patients with passive platysmal banding
■ Requires firm, toned skin and youthful subcutaneous tissue
■ Complications include dysphagia (rare).
ULTRASOUND SYSTEM
■ A microfocused ultrasound system (Ulthera System, Merz) for improved skin laxity and tightening of the lower face has been reported13:
■ Employs microfocused ultrasound to cause discrete focal heating of the dermis
■ Stimulates neocollagenesis and elastin remodeling
■ Largest clinical study to evaluate effectiveness of the technology
• At day 90, improvements reported by two thirds of patients and nearly 60% of blinded reviews
• Better outcomes in patients with BMI <30
• Local anesthesia/sedation suggested, because patients report pain
■ Technology requires judicial use in highly selected patients.
MEDICATION
In April 2015, the FDA approved an injectable drug (Kybella, Allergan) for treatment of submental fullness (also known as a double chin):
■ Deoxycholic acid, given as an injection
■ A naturally occurring molecule in the body that aids in breakdown and absorption of dietary fat
■ Indicated for improving the appearance of moderate to severe convexity or fullness associated with submental fat in adults
CAUTION: Kybella should not be injected in patients with dysphagia; into or in close proximity to the marginal mandibular branch of the facial nerve; or close to the salivary glands, lymph nodes, or muscles.
■ Causes injection site hematoma/bruising in most people (72% in clinical trials)
■ The formulation is nonhuman and nonanimal.
■ Causes destruction of fat cells when injected and cannot accumulate afterward
■ Currently the first and only nonsurgical treatment approved by FDA for submental fullness
■ Sold in Canada under the name Belkyra
■ Technique
• Injections are 2 mg/cm2 per dose.
• A single treatment consists of up to a maximum of 50 injections.
• Each injection is 0.2 ml (up to a total of 10 ml), spaced 1 cm apart.
• Up to six single treatments may be performed ≥1 month apart.
• In clinical trials, 68% responded to improvement with Kybella compared with placebo, based on validated physician and patient measurements.
SURGICAL OPTIONS FOR NECK REJUVENATION
Several isolated and combination procedures are available, and each is best suited according to anatomy and clinical presentation.
LIPOSUCTION14–20
■ Indications
• Best for isolated, younger patients (generally 20-30 years of age)
• Normal skin and subcutaneous quality with good tone
• Localized excess submental subcutaneous fat
• Not indicated for patients with subplastysmal fat (too deep for liposuction)
• Skin and subcutaneous pinch test is best assessment for selecting candidates.
• Should be no platysmal bands present at rest
• Isolated method, and can improve a short, fatty neck
• Can be combined with an open neck technique to ease subsequent surgical dissection
■ Technique
• General anesthesia is suggested, although local may be acceptable with caution.
• Patient must be supine, with neck extended.
• Incisions are in submental neck and/or (usually) behind earlobes.
• Lidocaine with epinephrine should be added to the wetting solution.
• A 2-3 mm single-hole cannula is adequate for suction-assisted liposuction (SAL).
• If ultrasonic suction (UAL) is used, a 2-3 mm solid probe set at 50% energy for no longer than 2-3 minutes is needed.
• UAL may be easier in thick, young, obtuse fatty neck.
• No drains are required if this is the only procedure.
• Jawline and lateral neck should be approached through earlobe incisions.
CAUTION: Stay above the platysma, or the marginal mandibular nerve may be injured by traction.
■ Preventing complications3
• Use short bursts of suction cannula strokes.
• Fan out from submental incision (Fig. 44-4).