9
Nasal and Nasal-Orbital-Ethmoid (NOE) Fractures
 Anatomy
Anatomy
The nasal area includes (Fig. 9–1)
• Nasal bone
• Frontal processes of the maxilla
• Nasal cartilages
• Nasal septum
• Quadrilateral cartilage
• Perpendicular plate of the ethmoid
• Vomer
Blood supply:
• Ophthalmic artery is the first branch of the internal carotid
• Anterior and posterior ethmoidal branches of internal carotid
• Facial artery branches
• Superior labial
• Internal maxillary branches of external carotid (sphenopalatine, greater palatine, and infraorbital)
External innervation:
• Nasociliary nerve V1
• Supratrochlear nerve V1
• Infraorbital nerve V2
Internal innervation:
• Anterior ethmoid nerve V1
• Greater palatine nerve – lateral wall
• Nasopalatine nerve V2
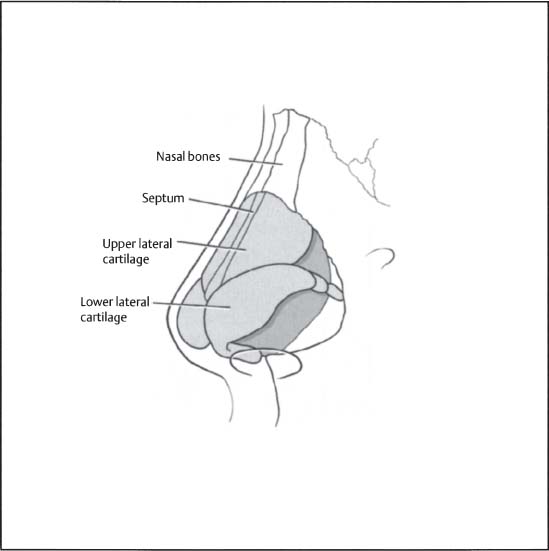
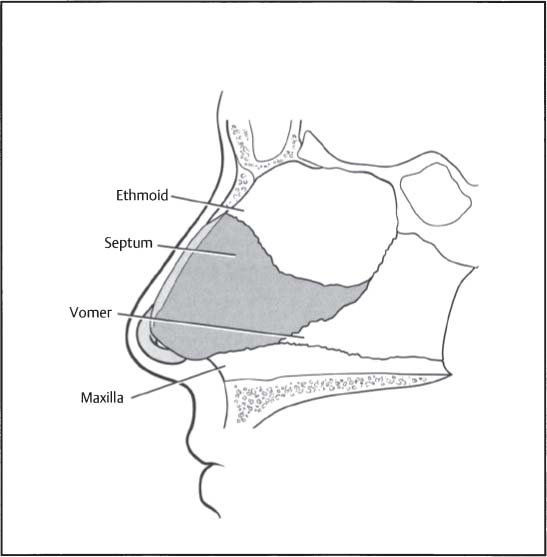
Figure 9–1 (A) Bony and cartilaginous vault anatomy. (B) Nasal septal anatomy.
 Nasal Fractures
Nasal Fractures
Physical Examination
Nasal fractures are usually a result of blunt trauma directly to the nose. Evaluation of the nose should take place in a well-lighted area with the patient comfortably seated and reclined at a 45-degree angle to facilitate inspection of both the external and internal nasal cavity. Suction, irrigation, nasal speculum, head light/handheld light, and cotton-tip applicators should be readily available. Common physical findings include
• Tenderness
• Crepitus
• Nasal deviation
• Mobility
• Epistaxis
• Airway obstruction
• Septal deviation
• Septal hematoma
• Saddle deformity
• Mucosal laceration
Septal Hematomas
Septal hematomas are caused by bleeding between the septum and mucosa. Diagnosis is made by direct visualization of a hematoma beneath the mucosa. Septal hematomas require immediate drainage and care in the acute setting. If left undrained, the accumulation of blood in the mucoperichondrium can lead to septal ischemia with potential septal necrosis. Complications include perforation, loss of dorsal support, and saddle deformity. Nasal septal hematomas should be drained appropriately with the proper pressure dressing applied (see Chapter 6, Fig. 6–4A). Packing should be removed on Day 3 to prevent sinusitis or toxic shock. Place patient on antibiotics.
Radiographic Evaluation
Plain films and CT scans (Fig. 9–2) are not absolutely necessary. Their necessity becomes more relevant if other injuries are suspected (e.g., nasal-orbital-ethmoid fractures [NOE], orbital floor fracture, intracranial bleed). If one has a low clinical suspicion for any other injury, nasal fractures in general do not require any radiography. In selected clinical scenarios, a nasal series (anterior and lateral view) can be ordered to aid in diagnosis and for documentation.

Figure 9–2 CT scan of nasal bone and septal fracture with orbital component.
Stranc-Robertson Nasal Fracture Classification (Fig. 9–3)
• Type I

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


