19
Upper Extremity Compartment Syndrome
Blunt crushing trauma is the most common cause of upper extremity compartment syndrome. Although less common, compartment syndrome can also occur in the hand and fingers. When confronting upper extremity injuries, it is important to closely monitor the patients for tissue ischemia and to correctly diagnose those who develop a true compartment syndrome. Delay in surgical intervention leads to devastating consequences. Compartment syndrome of the upper extremity requires urgent care due to its immediate sequela of muscle ischemia and long-term sequela of Volkmann contracture.
Increased compartment content or decreased compartment size leads to increased compartment pressures that cause tissue ischemia. Pay special attention to compartment pressures in cases of crush injury, severe soft tissue damage, fractures, intravenous infiltration, injection injuries, arterial insufficiency, burns, snakebites, lying on limb, and tight casts.
 Diagnosis
Diagnosis
The diagnosis of compartment syndrome is primarily a clinical one. The patient will have persistent pain that becomes worse with passive muscle stretching (a hallmark) or active flexion. The patient complains of diminished sensation, muscle weakness, and pain on palpation of the compartments. The presence of palpable pulses or Doppler ultrasound signals does not exclude increased intracompartmental pressures and compartment syndrome.
Cardinal Signs
• Persistent, progressive pain unrelieved with immobilization and elevation
• Pain with passive extension
 Passive muscle stretch test
Passive muscle stretch test
 Forearm
Forearm
 Dorsal compartment: Finger, thumb, and ulnar wrist extensors – test with passive wrist flexion
Dorsal compartment: Finger, thumb, and ulnar wrist extensors – test with passive wrist flexion
 Mobile wad: Extensor carpi radialis longus, extensor carpi radialis brevis, brachioradialis – test with passive wrist flexion
Mobile wad: Extensor carpi radialis longus, extensor carpi radialis brevis, brachioradialis – test with passive wrist flexion
 Volar compartment: Flexors of the fingers, thumb, and wrist – test by passive extension of the fingers, thumb, and wrist
Volar compartment: Flexors of the fingers, thumb, and wrist – test by passive extension of the fingers, thumb, and wrist
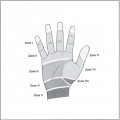
 Hand
Hand
 Intrinsic compartments: Keep MP joints in full extension and PIP joints in flexion. Pain with passive abduction and adduction of the fingers is diagnostically significant
Intrinsic compartments: Keep MP joints in full extension and PIP joints in flexion. Pain with passive abduction and adduction of the fingers is diagnostically significant
 Thumb adductor compartment: Pull and abduct the thumb
Thumb adductor compartment: Pull and abduct the thumb
• Diminished sensation
• Tense, tender forearm, or hand
Although a cool, pale, and pulseless extremity is often described in compartment syndrome, these are considered secondary signs and are often not present until late. Their absence should not delay surgery if cardinal signs are present.
Pressure Measurement
Use a Stryker needle (Fig. 19–1) or arterial line (Fig. 19–2) to measure compartment pressure. Forearm compartment pressures can be measured in the mobile wad and volar compartments with a Stryker needle:
< 25 mm Hg = normal − clinical observation, if worsens, repeat measurements

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


