Myocutaneous Island Flaps
Pectoralis Major Island Flap
( Fig. 12.1 )
Flap type:
Myocutaneous island flap of the axial pattern type (see Figs. 1.3 and 1.4 ).
Flap components:
Skin, subcutaneous fat, fascia, muscle (pectoralis major, vessels).
Use:
Myocutaneous island flap for reconstructing major defects in the neck and face (microvascular free transfer is possible).
Vascular pedicle:
The skin and muscle are supplied by the thoracoacromial artery, which is the second branch of the axillary artery past the scalene interval. The flap is supplied by the pectoral branches of the artery and their venae comitantes.
Position:
Supine.
Flap size:
Maximum 10 × 20 cm.
Flap elevation:
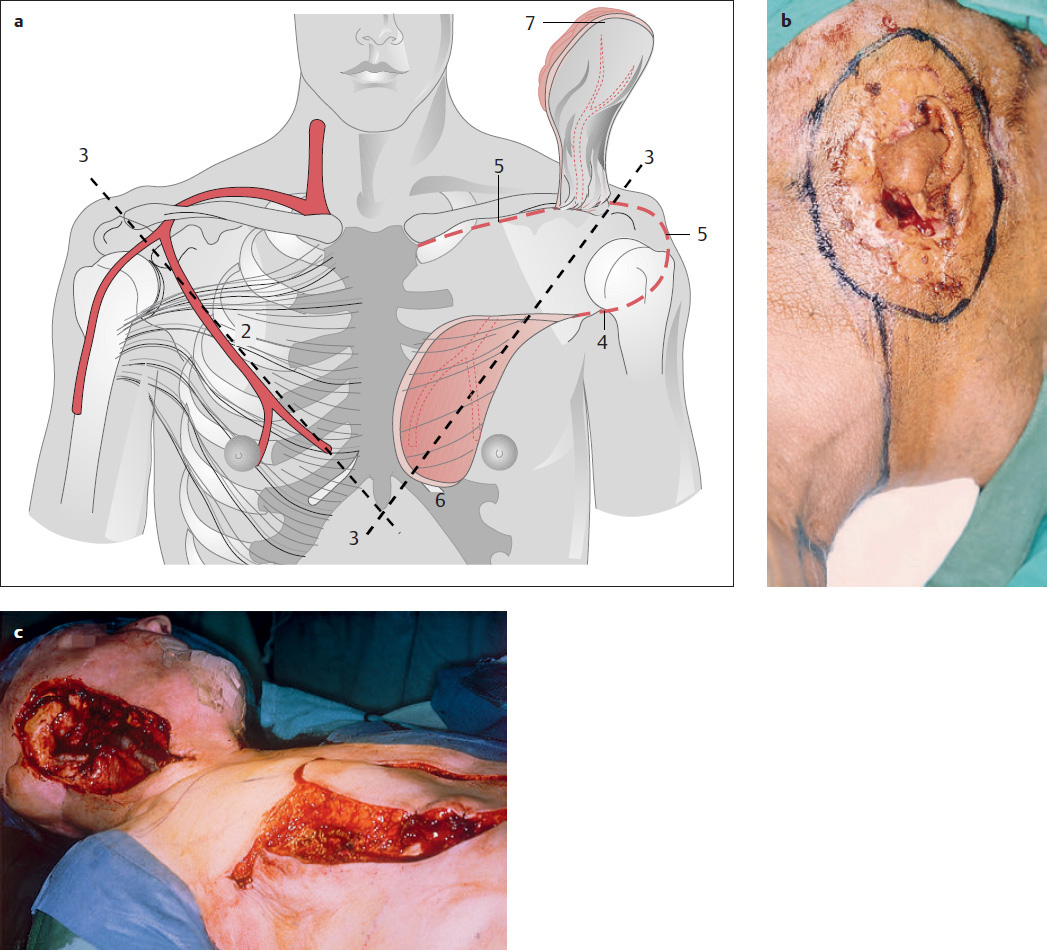
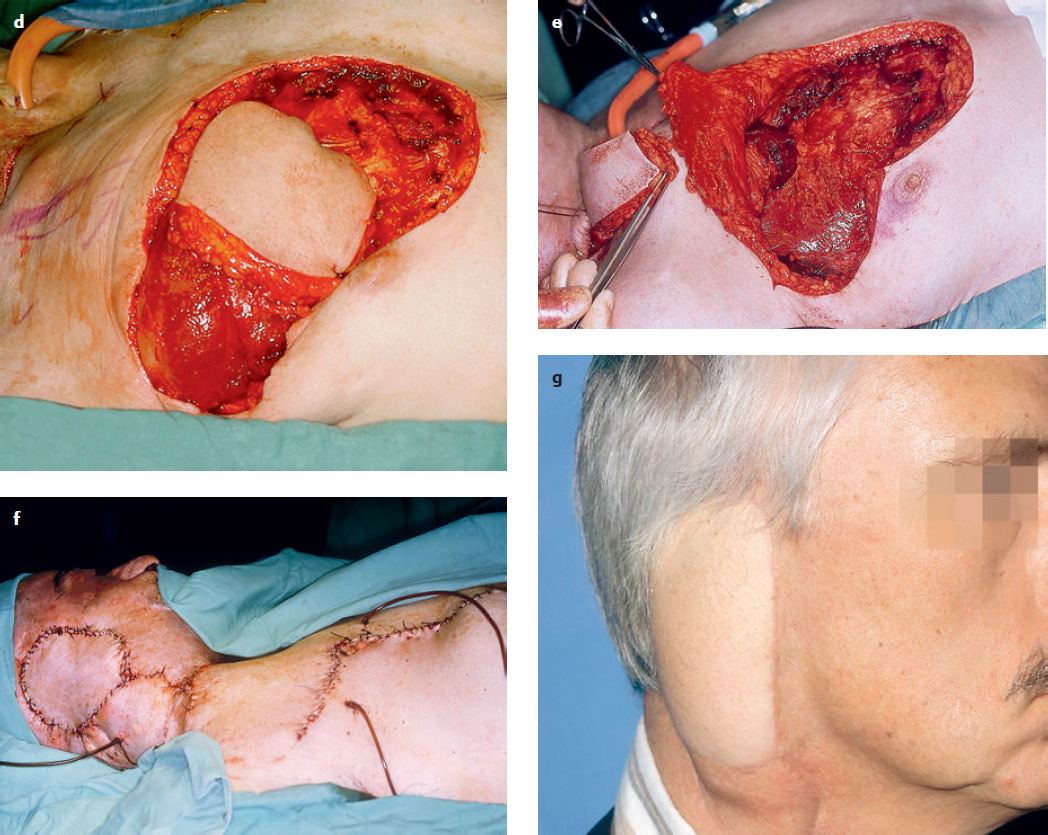
An imaginary line from the acromion of the scapula to the xiphoid process of the sternum marks the axis of the nutrient pectoral branches ( Fig. 12.1 , 3). The pivot point of the pectoralis major island flap is located just below the middle third of the clavicle. The pedicle must be long enough to reach from the pivot point at the clavicle to the recipient site in the head and neck region ( Fig. 12.1 , 7). The skin paddle should be placed medial to the nipple whenever possible. The incision is carried across the thorax ( Fig. 12.1 , 4), the skin is undermined to the lower incision for the subsequent transfer ( Fig. 12.1 , 4), and the skin, muscle, and underlying fascia are incised to outline the flap ( Fig. 12.1 , 6). The muscular portion of the flap should be slightly larger than the skin paddle. Next, the skin is sutured to the subcutaneous fat on the muscular fascia, to prevent shearing of the myocutaneous perforators. Proceeding from below upward, the pectoralis major muscle is elevated from the chest wall on its nutrient vascular pedicle, along with the deep muscular fascia. The arc of rotation can be increased by releasing the humeral and clavicular muscle attachments, leaving about a 4-cmwide muscle pedicle to protect the nutrient vessels. The skin outline of a deltopectoral flap should be preserved ( Fig. 12.1 , 5) so that this flap will also be available if needed. When the island flap has been elevated to the clavicle, it is rotated 180° and carefully tunneled under the skin and over the clavicle to reach the defect ( Fig. 12.1 , 7).
Indications and advantages:
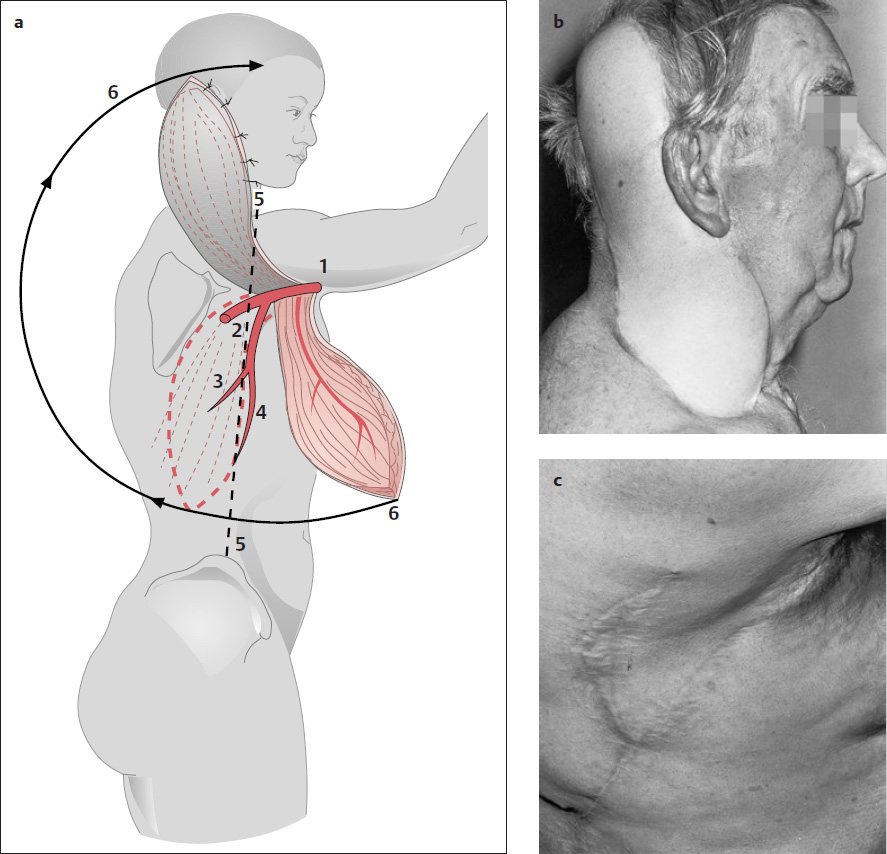
The pectoralis major island flap can be used in reconstructions of the pharynx, tongue, face, and neck, and especially to cover the carotid artery when this vessel is at risk because of prior irradiation. Tumor excision and reconstruction can be completed in one operation ( Fig. 12.1b–g ). We find that the vascular pedicle has a consistent anatomic course. Direct closure is possible in most patients. There is no need to reposition the patient when raising the flap. The pectoralis major flap can be combined with a deltopectoral flap ( Fig. 12.1 , 5) or a latissimus dorsi island flap (see Fig. 12.2 ). It can also be used as a purely muscular flap or myofascial flap without a skin paddle.
Disadvantages and complications:
A large donor defect will require skin grafting. Esthetic objections are most common in women, owing to breast distortion, and the incision should be placed in the inframammary fold whenever possible. Thick subcutaneous fat and muscle bulk make it difficult to model the flap. Long-term results can be marred by volume reduction due to shrinkage and scarification.
Heavy body hair in male patients limits the indications for this flap in reconstructions of the oral cavity and pharynx.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


