The authors provide a review of treatment of the mutilated hand, discussing the effect of injury on soft tissue loss, intrinsic and extrinsic musculature, paravascular structures, tendons, and the bony skeleton. The authors review functional loss and restoration.
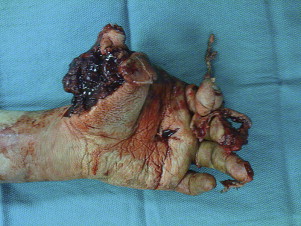
Mutilated hand injuries are one of the most challenging reconstruction problems than can confront hand surgeons ( Fig. 1 ). Injuries occur by a variety of mechanisms, including crush, avulsion, friction, or sharp trauma. Because of the nature of the trauma and the intricate balance of hand structures, these injuries may result in devastating compromise of function of the entire extremity and impair the quality of daily living. Mutilating injuries not only involve soft tissue loss but also damage the intrinsic and extrinsic musculature, paravascular structures, tendons, and the bony skeleton, requiring complex problem solving to restore function.
The American Medical Association has developed the guidelines for the evaluation of permanent impairment, which described the functional contribution of each digit to the hand, upper extremity, and the entire body. Loss of the thumb results in a 40% loss of function and 25% loss of total body function. Although other digits are not rated as high, each one has its specific functional contribution. The radial digits are important for key and chuck pinch, whereas the ulnar digits are more important for grip strength and strong grasp. Compromise to any digit translates to a functional deficit with enormous implications for individuals who work with their hands.
The proper evaluation of outcomes includes not only the assessment of overall function but also the ability to perform the desired work and activities of daily living, pain, total range of motion, sensation, and grip strength. These outcomes paired with patient and physician priorities direct the reconstructive efforts.
Initial evaluation
Although the mangled extremity is often one of the most obvious of injuries, each patient should undergo an initial trauma evaluation to rule out more life-threatening injuries. After stabilization and initial resuscitation, the physician can further address limb salvage and functional reconstruction. The functional restoration of the upper extremity relies on many factors. The patient’s premorbid functional status, handedness, occupation, general medical status, and socioeconomic status are all important in treating the patient. Comorbidation, such as diabetes and heart and pulmonary disease, can complicate acute medical and surgical care but can also be contributing factors to compliance with postoperative therapy.
Functional Outcome
The functional outcome depends ultimately on various factors such as mechanism of injury, ischemia time, contamination, and tissue loss. The final outcome also depends on the ability of secondary procedures to reconstruct tissue, release contractures and adhesions, or restore nerve, muscle, or tendon responsibility.
If tissue is amputated and replantation is contemplated, the ischemia time will be critical. An attempt should be made to instruct the field staff on proper care during transport of the amputated part. Immediate cooling of any amputated parts should be achieved by wrapping the parts in moist saline gauze and placing them into a sealed bag on ice. Those amputated parts that have less muscle can withstand greater ischemia times. The degradation products of muscle can be detrimental to life. These byproducts include high potassium and myoglobin levels that can disrupt cardiac and kidney function, respectively. There are no muscles within digits; therefore, ischemia is well tolerated in digits. The recommended ischemia times are 12 hours for warm and 24 hours for cold ischemic digits and 6 hours for warm and 12 hours cold ischemia for other more proximal replants that involve greater amounts of muscle. Although longer times have resulted in success, such as 94 hours of cold ischemic digits, 54 hours of cold ischemia in the hand, and 42 hours of warm ischemia, these prolonged ischemia times are not globally achievable or advisable.
Surgery for the mutilated hand
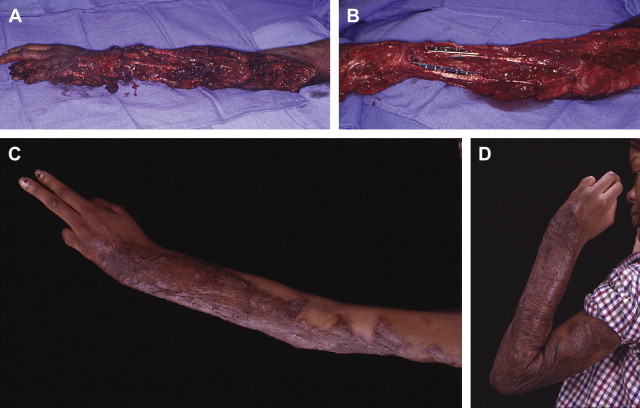
The mainstay of the initial surgery should include irrigation, debridement, and treating the wound like a pseudotumor ( Fig. 2 ). The wound is thoroughly debrided of any devitalized tissue or contamination. The vascular status can be evaluated not only through color and skin turgor but also through direct bleeding of surrounding tissues. Reconstructive efforts can be delayed until a second- or third-look procedure is performed to make sure that contamination or infection is minimized. Vascular compromise may require arterial repair or vein transplants to the initial surgery. Nerve repairs should also be performed with microsurgical assistance. Other aspects of microsurgical care can be delayed, including definitive coverage with free tissue transfer.
Free Tissue Transfers
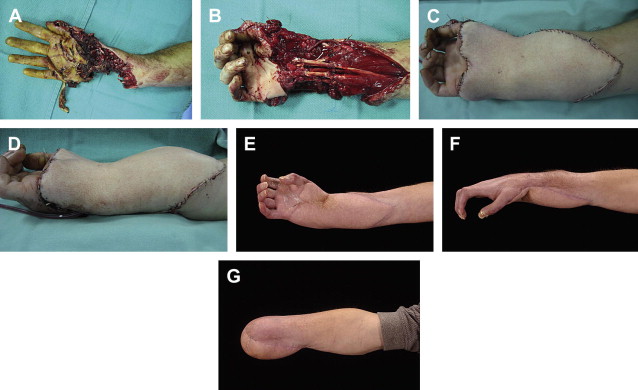
Free tissue transfers at the time of the initial surgery are rarely, if ever, indicated. The exceptions to that rule is the use of spare parts, in which amputated segments of the extremity can be used as a free tissue transfer to close exposed structures ( Fig. 3 A–C). In this scenario, the amputated part was otherwise to be discarded, and, therefore, its potential as spare parts should be used. Replantation is another indication for emergent microsurgical techniques. In multiple digit replants, the current philosophy is to perform structure by structure as opposed to digit by digit. This method seems to optimize operative time.
Reconstruction
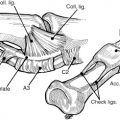
The principles of reconstruction of the various tissues in the mutilated upper extremity should follow those principles identified for each individual structure within the hand. That is, all the important principles of repair and reconstruction apply to individual tissues such as tendons, nerves, arteries, bone, and skin. Bony fixation proceeds soft tissue repair ( Fig. 4 ). The optimum treatment of fractures is dictated somewhat by the pattern and location of the fracture. However, surgeon preference and comfort level is probably the most important factor because each type of fixation affects its own inherent advantages and disadvantages ( Table 1 ). Tendon repair and/or reconstruction proceeds soft tissue coverage but need not be delayed for secondary surgery. Primary tendon transfers and repair affect early outcomes with fewer secondary procedures and foster return to function.
| Fixation | Advantages | Disadvantages |
|---|---|---|
| Kirschner wire & interosseous wire |
|
|
| Tendon band |
|
|
| Plates |
|
|
| Lag screws |
|
|
| External fixation |
|
|
Devastating injury to multiple tissues usually portends a rather poor prognosis in terms of return to normal function (see Fig. 3 ). Surgeons should adhere to the initial principles but fully understand and plan for secondary procedures that may be warranted. These secondary procedures may be required to release scar tissue, improve range of motion, provide soft tissue coverage, counteract contractures, restore sensation, and provide bony stabilization. The surgeon should start to formulate the definitive surgical architectural plan for subsequent reconstructions even at the initial surgery ( Figs. 5–7 ).
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


