Large cutaneous tumors of the head and neck provide challenges for complete excision and optimal reconstruction. Collaborative intraoperative Mohs micrographic surgery offers efficient and reliable extirpation of large cutaneous malignancies of the head and neck and immediate reconstruction of resultant defects.
Nonmelanoma skin cancers are the most common malignancies in the United States and most frequently occur in areas of direct sun exposure, such as the head and neck regions. Tumors in so-called high-risk areas as well as recurrent tumors have been successfully approached using Mohs micrographic surgery (MMS) with established advantages over other methods of resection and margin control. However, large tumors, aggressive pathology, and involvement of multiple aesthetic units or critical structures can complicate excision under local anesthesia and warrant extensive reconstruction.
As a result, extensive or massive cutaneous tumors of the head and neck are traditionally approached in the operating suite under general anesthesia where excision with predetermined margins is easily accomplished and reconstructive capabilities are readily available. In such instances, MMS is rarely used and frozen-section analysis is commonly employed to ensure marginal clearance, albeit with known compromise of accuracy and consequently inferior tumor control. Given these limitations, periods of observation for recurrence have been advocated prior to definitive reconstruction of defects, resulting in additional patient morbidity and psychosocial compromise.
The seemingly obvious need for optimal margin clearance when managing complex, massive, or multiple cutaneous malignancies necessitates a shift in current resection paradigms. As a result, the authors have begun a unique and now routine collaborative approach to large tumors, which concurrently employs multiple subspecialties to ensure both optimal oncologic management and appropriate aesthetic and functional reconstruction. Currently at the authors’ institution, dermatologic surgeons, facial plastic surgeons, head and neck surgeons, and additional subspecialties manage tumors in a single operative setting. This method of intraoperative Mohs micrographic surgery (IMMS) provides efficient and reliable extirpation of large tumors and allows for immediate reconstruction of complex defects.
Role of Mohs micrographic surgery in large tumors
Mohs micrographic surgery is advantageous in the treatment of head and neck cutaneous malignancies for its ability to effectively evaluate the tumor margins while simultaneously preserving tissue. Marginal control is paramount in reducing the potential for metastatic disease, recurrence, and increasing overall and disease-free survival. Several methods of treatment have been employed for head and neck cutaneous malignancies, including conventional excision, MMS, cryosurgery, and electrodessication and curettage. Only conventional excision and MMS are recommended, as the other methods cited result in operator-dependent outcomes and difficulty yielding histological evidence of adequate margins. Conventional excision with adequate gross margins is commonly employed by nondermatologists for large or recurrent basal cell carcinomas (BCC) and squamous cell carcinomas (SCC). Current recommendations cite 4-5 mm surgical margins for well-defined small basal and squamous cell carcinomas and 4-15 mm margins for large BCC or SCC to achieve clearance in approximately 95% of tumors. Intraoperative frozen-section analysis is often employed to confirm negative margins during conventional resection of large tumors in the operating suite. However, frozen-section analysis can be dependent upon artifact, proper orientation, sectioning method, and completeness of section. Frozen-section analysis in the setting of recurrent facial cutaneous BCC reports a 72% rate of accuracy ; whereas, MMS reports 5-year cure rates of up to 98.9% for both primary and recurrent BCC and SCC.
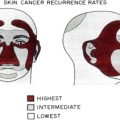
MMS has been established as the gold standard for excision of higher-risk cutaneous malignancies, including large cutaneous tumors (>2 cm in diameter). Regardless of size, high-risk clinical features also include tumors that are recurrent, located in areas with high risk of recurrence (midface, ear, and lip), and have ill-defined boundaries or aggressive pathology. In such cases, the improved cure rate over conventional excision is most certainly attributable to the ability of MMS to assess 100% of the excised tumor margin as opposed to the estimated 1% of margin directly evaluated with traditional surgical excision and paraffin-section margin assessment. Optimal management of large (>5 cm), so-called giant BCC and large SCC is not well established. Recent data indicates that Mohs excision of large BCC and SCC could be advantageous for definitive tumor control, but is not without challenges and potential limitations.
Challenges in management of large tumors
Large cutaneous tumors of the head and neck provide unique challenges not only for Mohs clearance and adequate extirpation but also for functional and aesthetic reconstruction. Often, large tumors require increased operative time and multiple sections, which may be difficult to accomplish in an office-based setting. Longer operative times and the potential need for more extensive resection may also hinder the ability of patients to tolerate excision under local anesthesia. Necessity for deeper resection or resection involving critical structures, including bone, deep tissues, eyelid, orbit, or nasal mucosa, may also obviate office-based excision. Tumors with nodal metastasis, parotid extension, bone invasion, or intracranial extension along nerve branches may not be cleared with office-based MMS. Also, if several aesthetic subunits are involved, the resultant wound may require more complex reconstructive techniques than are available in an office-based setting and may require general anesthesia to accomplish them. Finally, resection of large tumors requiring delayed reconstruction with or without general anesthesia, or multiple-staged formalin-fixed tissue Mohs resections (so-called slow Mohs) are disadvantageous because of the inconvenience to patients, aesthetic concerns with a large wound, and potential risk for secondary infection or wound contracture. Despite these limitations of office-based MMS in the setting of large tumors, the collaborative approach of IMMS, which the authors advocate, offers the advantages of total marginal assessment and clearance of large and complicated tumors coupled with the ability to immediately and efficiently reconstruct the resultant defect. Therefore, extensive tumors with or without deep invasion, those involving critical structures or multiple aesthetic subunits are ideal types to approach with a multidisciplinary technique. In properly selected patients, this approach can minimize the number of procedures, operative time, and potential morbidity for patients.
Challenges in management of large tumors
Large cutaneous tumors of the head and neck provide unique challenges not only for Mohs clearance and adequate extirpation but also for functional and aesthetic reconstruction. Often, large tumors require increased operative time and multiple sections, which may be difficult to accomplish in an office-based setting. Longer operative times and the potential need for more extensive resection may also hinder the ability of patients to tolerate excision under local anesthesia. Necessity for deeper resection or resection involving critical structures, including bone, deep tissues, eyelid, orbit, or nasal mucosa, may also obviate office-based excision. Tumors with nodal metastasis, parotid extension, bone invasion, or intracranial extension along nerve branches may not be cleared with office-based MMS. Also, if several aesthetic subunits are involved, the resultant wound may require more complex reconstructive techniques than are available in an office-based setting and may require general anesthesia to accomplish them. Finally, resection of large tumors requiring delayed reconstruction with or without general anesthesia, or multiple-staged formalin-fixed tissue Mohs resections (so-called slow Mohs) are disadvantageous because of the inconvenience to patients, aesthetic concerns with a large wound, and potential risk for secondary infection or wound contracture. Despite these limitations of office-based MMS in the setting of large tumors, the collaborative approach of IMMS, which the authors advocate, offers the advantages of total marginal assessment and clearance of large and complicated tumors coupled with the ability to immediately and efficiently reconstruct the resultant defect. Therefore, extensive tumors with or without deep invasion, those involving critical structures or multiple aesthetic subunits are ideal types to approach with a multidisciplinary technique. In properly selected patients, this approach can minimize the number of procedures, operative time, and potential morbidity for patients.
Related posts:
 Mohs Micrographic Surgery Technique
Mohs Micrographic Surgery Technique
 Mohs Surgery for Squamous Cell Carcinoma
Mohs Surgery for Squamous Cell Carcinoma
 Flaps and Grafts Reconstruction
Flaps and Grafts Reconstruction
 Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
 Nonsurgical Treatment of Nonmelanoma Skin Cancer
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Nonsurgical Treatment of Nonmelanoma Skin Cancer
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


