Multi-Island Free Radial Forearm Flap for Reconstruction of The Nasal Lining
R. L. WALTON
EDITORIAL COMMENT
Total nose reconstruction has reached a level of spectacular development (1, 2, 3, 4), particularly with the clinical examples demonstrated by Walton and Burget. Nasal lining is a most important step prior to the placement of the cartilaginous framework and the overlying skin. The multi-island free radial forearm flap demonstrated here provides the nasal lining quite well. Obviously, it requires a considerable amount of planning.
The first stage for reconstruction of total and subtotal nasal defects is the microsurgical transfer and restoration of the nasal lining and adjacent cheek and upper lip elements, using a multi-island free radial forearm flap. Two months following microsurgical transfer of the nasal lining flap, nasal reconstruction proceeds with application of a cartilage framework and a paramedian forehead flap.
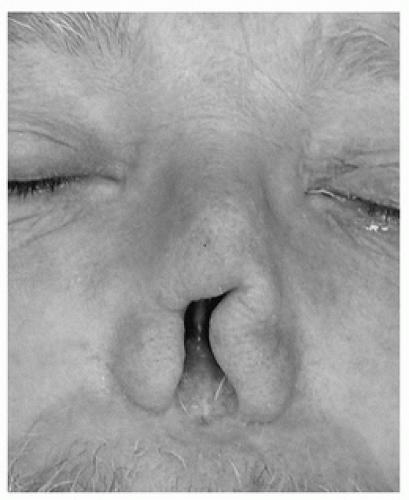 FIGURE 71.1 Preoperative frontal view of subtotal nasal defect showing composite loss of nasal tip, columella, alae, anterior septum, and vestibular lining. |
INDICATIONS
Restoration of major nasal loss involving overlying skin and underlying nasal passages including support and lining requires staged reconstruction. A microsurgical approach is used for restoration of the nasal lining prior to external nasal cover reconstruction. Following defect evaluation and careful discussion with the patient, the operative sequence is initiated (Figs. 71.1, 71.2, 71.3).
FLAP DESIGN AND DIMENSIONS
Preoperatively, an Allen test is performed to ensure adequate hand perfusion via the ulnar vascular pedicle. The nasal site is dissected first, with excision of the remnant scar and any skin grafts, to recreate the original defect (Fig. 71.4). Templates of the missing vestibular and adjacent lip and cheek defects are made of foil from surgical suture packets and then transferred to the forearm, where they are aligned to the radial vascular pedicle as separate islands. The radial side of the flaps is positioned to overlap the vascular pedicle by no more than 5 mm, so as to place the pedicle out of harm’s way during subsequent procedures. For the vestibular lining element, we have found it helpful to orient the vascular pedicle at the cephalic edge, so as to allow unsullied access to the nasal tip and vestibule for placement of the supporting cartilage grafts and for sculpting (Fig. 71.5).
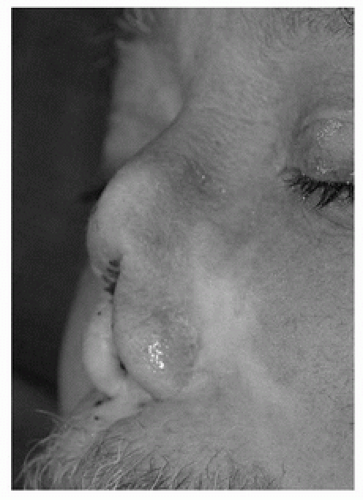 FIGURE 71.2 Preoperative three-quarter view depicting subtotal nasal defect. |
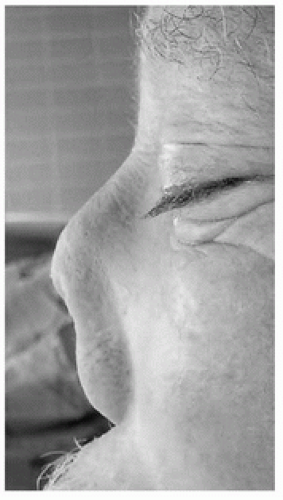 FIGURE 71.3 Preoperative lateral view depicting subtotal nasal defect. |
 FIGURE 71.4 Preparation of the nasal site. Contracted scar has been removed, and the wound and adjacent nasal elements are repositioned anatomically.
Related posts: Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction Nasalis Musculocutaneous Sliding Flaps for Nasal Tip Reconstruction
 Oral Mucosal Flaps for Septal Reconstruction Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap) Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Scapular and Parascapular Flaps Scapular and Parascapular Flaps
 Platysma Musculocutaneous Flap to The Lower Lip Platysma Musculocutaneous Flap to The Lower Lip
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|