36
Morphea and Lichen Sclerosus
Morphea (Localized Scleroderma)
• It is distinct from systemic sclerosis (SSc; see Chapter 35) in that morphea is not associated with sclerodactyly, Raynaud’s phenomenon, nailfold capillary abnormalities, or internal organ involvement.
• Morphea does not transition into SSc, except for a few rare case reports.
• Equal prevalence in adults and children; more common in females and Caucasians.
• Classified based on clinical presentation, with five major variants recognized (see Fig. 35.1; Table 36.1).
Table 36.1
Approach to the treatment of morphea.
Treatment is most effective in active, inflammatory lesions. Topical monotherapy should not be used if any of the following are present: progressing functional impairment, joint contractures or involvement across joints, linear facial involvement.
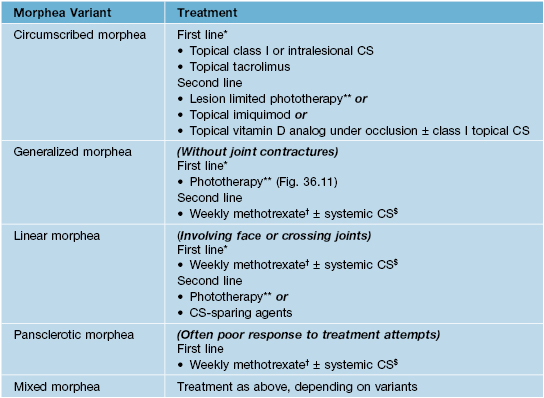
* If not improved after ~8 to 10 weeks, progress to next line of therapy.
** Phototherapy choice based on local availability (BB-UVA, UVA1, NB-UVB, PUVA); NB-UVB more effective for superficial lesions and UVA1 more effective for deeper lesions.
† Weekly methotrexate doses: adults, 15–25 mg/week; children, 0.3–0.4 mg/kg/week.
$ Especially for early/progressive lesions; pulsed > daily dosing.
BB-UVA, broadband ultraviolet A light phototherapy; UVA1, narrowband ultraviolet A light phototherapy; NB-UVB, narrowband ultraviolet B light phototherapy; PUVA, psoralens plus ultraviolet A light phototherapy.
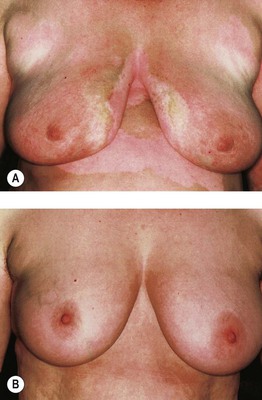
• Early morphea lesions present as erythematous to violaceous patches and plaques (Fig. 36.1); they then evolve into sclerotic (often ivory-colored), hairless, anhidrotic plaques with variable degrees of dyspigmentation (Fig. 36.2).


• Circumscribed (plaque) morphea is the most common variant in adults, presenting with ≤3 discrete indurated plaques; the latter favor the trunk and tend to develop in areas of pressure (e.g. hips, waist, and bra line in women); superficial and deep variants (morphea profunda) exist (Fig. 36.3).


• Generalized morphea is a rare variant that presents with >3 indurated plaques larger than 3 cm and/or involving ≥2 body sites; spares the face and hands (see Fig. 36.11); more likely to have a (+) ANA and systemic symptoms.
• Linear morphea is the most common variant in children and may cause a significant degree of morbidity because of ocular involvement and occasionally CNS involvement in the head variant (Fig. 36.4) or muscle atrophy, discrepancies in limb length, and joint contractures in the limb variant (Fig. 36.5).






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


