Cutaneous squamous cell carcinoma (SCC) is the second most common human cancer and can behave aggressively. Mohs micrographic surgery offers the highest cure rates for high-risk SCCs and is particularly useful for SCCs on challenging anatomic sites.
Cutaneous squamous cell carcinoma (SCC) is a neoplasm of keratinizing cells that shows malignant characteristics, including anaplasia, rapid growth, local invasion, and metastatic potential ( Fig. 1 ). More than 250,000 cases of SCC are diagnosed in the United States each year, making it the second most common human cancer after basal cell carcinoma (BCC). The biologic behavior of SCC is determined by several variables. The overall invasiveness and depth of the neoplasm is significant when determining the risk of recurrence after treatment. SCCs that invade the reticular dermis and subcutis tend to recur if not properly treated. Immerman and coworkers observed a 20% incidence of recurrence in 86 subjects with invasive SCC. Degree of cellular differentiation is also important, with poorly differentiated neoplasms showing increased rates of recurrence. SCC that is incompletely treated or neglected can result in metastases ( Fig. 2 ).

Squamous cell carcinoma in situ tends to arise in association with preexisting actinic keratosis, most commonly on sun-damaged skin. Although SCC in situ is considered to have little to no risk of metastasis, invasive SCC can metastasize and can originate in neglected SCC in situ. The incidence of metastasis of invasive SCC is 3% to 5%. A higher incidence (10%–30%) is associated with SCC arising on mucosal surfaces (lip, genitalia) and on sites of prior injury (scars, chronic ulcers).
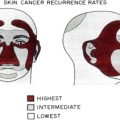
In a review of studies of SCCs treated over a 30-year period, Rowe and colleagues correlated risk for local recurrence and metastasis with treatment modality, prior treatment, location, size, depth, histologic differentiation, evidence of perineural involvement, precipitating factors other than ultraviolet light, and immunosuppression. They found that with tumors greater than 2 cm, recurrence rates doubled from 7.4% to 15.2%. In addition, they demonstrated that tumors less than 4 mm in depth were at low risk for metastasis (6.7%) compared with tumors greater than 4 mm in depth (45.7%). Locally recurrent SCCs showed an overall metastatic rate of 30% with high rates of metastasis in the context of local recurrence in skin (25.0%), lip (31.5%), and ear (45.0%). Poorly differentiated SCC metastasized more frequently (32.9%) than well-differentiated SCC (9.2%). SCC arising on sun-exposed skin recurred at a rate of 7.9% and metastasized at a rate of 5.2%. Recurrence rates were increased in SCC on the lip (10.5%) and ear (18.7%), as were metastatic rates from the lip (13.7%) and ear (11%). SCCs with perineural invasion (PNI) recurred in almost one-half of cases (47.2%) and showed a similar rate of metastasis (47.3%).
Patients who are immunosuppressed are a special high-risk group and are thought to have a 5- to 20-fold increase in the incidence of SCC compared with the general population, with a reversal of the SCC/BCC ratio from 0.25:1 to 3.0:1. The number of SCCs per patient is increased and the age at initial presentation is decreased (see later discussion of SCC in organ transplant recipients). Rowe and colleagues found that in patients who are immunosuppressed, the overall rate of metastasis was 12.9%.
Therapy for SCC should be selected on the basis of the size of the lesion, anatomic location, depth of invasion, degree of cellular differentiation, and history of previous treatment. There are 3 general approaches to the treatment of SCC: (1) removal by traditional excisional surgery or Mohs micrographic surgery (MMS), (2) destruction by curettage and electrodesiccation, and (3) radiation therapy. In this article the authors review the use of Mohs micrographic surgery for cutaneous squamous cell carcinoma and discuss its role as the treatment of choice for select squamous cell cancers.
Mohs micrographic surgery
Mohs micrographic surgery facilitates optimal margin control and conservation of normal tissue in the management of nonmelanoma skin cancer. Individuals specially trained in the technique perform MMS in an office setting under local anesthesia. Briefly, following gentle curettage, a tangential specimen of tumor with a minimal margin of clinically normal-appearing tissue is obtained, precisely mapped, and processed immediately by frozen section for microscopic examination. Optimal margin control is obtained by examination of the entire perimeter of the specimen and contiguous deep margin. Meticulous mapping allows for directed extirpation of any remaining tumor. A key defining feature of MMS is that the surgeon excises, maps, and reviews the specimen personally, minimizing the chance of error in tissue interpretation and orientation. MMS has gained acceptance as the treatment of choice for recurrent skin cancers as well as primary skin cancers located on anatomic sites requiring maximal tissue conservation for preservation of function and cosmesis.
MMS is indicated in cases of primary or recurrent SCC because this modality allows conservation of normal tissue with preservation of function and enhanced cosmesis. MMS is also superior to other forms of treatment with regard to local recurrence. Recurrence rates with MMS are superior to those obtained with traditional excisional surgery in primary SCC of the ear (3.1% vs 10.9%), primary SCC of the lip (5.8% vs 18.7%), recurrent SCC (10.0% vs 23.3%), SCC with PNI (0% vs 47%), SCC greater than 2 cm (25.2% vs 41.7%), and poorly differentiated SCC (32.6% vs 53.6%). MMS has proven useful in SCC involving the nail unit, and has been used as a limb-sparing procedure in cases of SCC arising in osteomyelitis. MMS is indicated for invasive lesions, poorly differentiated lesions, and for lesions occurring on high-risk anatomic sites or sites where conservation of normal tissue is essential for preservation of function or cosmesis.
In addition to providing the highest cure rates for the most aggressive SCCs, MMS remains cost effective when compared with other modalities. For example, the overall cost for MMS and immediate reconstruction by a fellowship-trained Mohs micrographic and reconstructive surgeon may be 3-fold less than that performed by a colleague from an allied surgical subspecialty in an ambulatory surgical center. Five-year recurrence rates also remain lower for patients treated using the Mohs technique.
Pugliano-Mauro and Goldman reviewed 215 subjects with 260 high-risk cutaneous SCCs treated with MMS in a single-center retrospective study, and considered rates of recurrence, metastasis, and death. A total of 77% of the subjects were men and 23% were women. The average age was 70.6 years. Twenty percent of the subjects were immunosuppressed. Mean follow-up was 3.9 years. There were 3 local recurrences (1.2%). Six (2.3%) tumors metastasized, with one fatality from disease. In general, prompt recognition of metastatic disease allowed for curative therapy. Twelve (4.6%) tumors involved named nerve trunks and in 8 of these cases, adjuvant radiation therapy was employed (adjuvant radiotherapy was reserved for large-nerve perineural disease). A total of 75% of the subjects went on to develop another cutaneous SCC, and 7.7% developed subsequent malignant melanoma, suggesting that once a patient has one high-risk SCC they are likely to develop secondary primary SCC and melanoma. The investigators concluded that MMS is an effective treatment for high-risk cutaneous SCC, providing a low recurrence rate and a low disease-specific mortality. This study is the largest single-center study of high-risk SCC supporting the use of MMS.
Jumbusaria and colleagues reported variation in perioperative management in patients with PNI or otherwise high-risk SCC. The authors at this time do not routinely recommend sentinel lymph node biopsy for cutaneous SCC. However, the authors do refer patients with PNI for evaluation for radiation therapy and recommend evaluation of patients with PNI by a radiation oncologist with expertise and experience treating cutaneous SCC (see later discussion of perineural invasion).
Related posts:
 Mohs Micrographic Surgery Technique
Mohs Micrographic Surgery Technique
 An Overview of Mohs Micrographic Surgery for the Treatment of Basal Cell Carcinoma
An Overview of Mohs Micrographic Surgery for the Treatment of Basal Cell Carcinoma
 Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
 Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


