Mohs micrographic surgery is a valuable option for the treatment of melanoma in situ, especially lesions of the lentigo maligna subtype that are clinically ill defined. Complete peripheral margin assessment of a tumor’s borders by means of frozen or permanent sections can help reduce the surgical defect size and maximize cure rate as compared with standard excision with preset 5-mm margins. This article reviews the different variations of Mohs micrographic surgery that are currently used for melanoma in situ.
Mohs micrographic surgery (MMS) was first described as a treatment for melanoma by Frederick Mohs in 1950, as a method to achieve complete peripheral margin examination (CPME) of a tumor using the “fixed tissue” zinc chloride chemical fixation technique. His method was tissue-sparing and had a 5-year cure rate of 35%, similar to that obtained by radical surgery. Twenty cases were described, spanning different subtypes and stages of melanoma, some of which already had clinical lymph node involvement. In a later article, Mohs showed that when comparing melanomas of a similar Clark level, MMS actually had superior 5-year cure rates compared with radical surgery. Of note, in both studies Mohs removed an additional 1- to 3-cm margin after a microscopic melanoma-free plane was obtained, to mitigate the effects of satellite and lymphatic spread. However, even with these extra margins, the MMS approach was still considered relatively tissue-sparing at a time when margins of 5 cm or more were routinely employed in melanoma surgery.
MMS depends on several principles for its success. These factors include: (1) the existence of a contiguous tumor growth pattern to avoid a false-negative margin; (2) tumor cells must be easily mapped and identifiable in the sections and be differentiated from nontumor cells; and (3) total processing time for excision, CPME, and defect repair should be within a reasonable time frame. Therefore, with the goal of achieving a local cure, the authors review how MMS is currently applied in the treatment of melanoma in situ (MIS).
There are several variations in techniques and application of CPME for MIS. While the use of MMS for nonmelanoma skin cancer has been well established, its use for MIS is less universally practiced. The challenges of histologic examination of atypical melanocytes at the margin make interpretation by frozen section difficult, especially on chronically sun-damaged skin. The current gold standard for interpretation of atypical melanocytes is by paraffin permanent sections, and therapeutic success is ultimately determined by recurrence rates based on long-term clinical follow-up.
Rationale for surgery
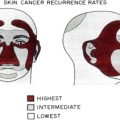
Lentigo maligna (LM) is the most prevalent subtype of MIS (>75%), and its incidence is increasing, especially in the elderly white male population. Lentigo maligna melanoma (LMM), the invasive counterpart to LM, comprises 12% of all melanomas. LM and LMM present clinically as an asymmetric and irregularly pigmented patch located on chronically sun-damaged skin. Margins can be poorly defined, with extensive subclinical disease beyond the area of pigmentation. The majority of LMs occur on cosmetically sensitive areas such as the head and neck region, especially on the cheeks, where tissue conservation of normal skin is a priority. LM can often involve important functional areas such as the eyelids, and individual tumors may cover large surface areas of the face. Lesions often present clinically as variations of tan, dark brown, or black colors within a large patch, and it is the darker regions or an area with thickening that is usually sampled by biopsy for diagnosis. LM typically undergoes a prolonged centrifugal horizontal growth phase along the dermal-epidermal junction, which can at some point progress to LMM, with the development of invasive foci. LM is treated to prevent this progression to LMM, which occurs in a range of 2% to 50% of cases. Once LMM develops, prognosis is similar to other melanomas of the same depth and staging.
Although there may be times when surgery is contraindicated, complete surgical excision is the standard of care for biopsy-proven LM. It is especially important to examine the entire lesion by histopathology to rule out an invasive component. A review of the literature finds that a range of 5% to 67% of lesions initially determined to be LM by biopsy examination turn out to contain foci of invasive disease when the remainder of the lesion is examined after therapeutic excision ( Table 1 ). The potential for missing an invasive component in these instances averages 21%. Although not yet formally studied, it seems reasonable that larger tumors are more likely to contain an unseen invasive focus, because the initial biopsy represents a smaller percentage of the entire lesion. Al-Niaimi and colleagues. reviewed 65 cases and reported that 3-mm or 4-mm punch biopsies were the most commonly used method to diagnose LM. While their recommendation to use incisional biopsies or larger punch biopsies would lower the incidence of missing an invasive component, the emphasis should still be placed on complete excision and histologic examination of the entire specimen to rule out invasive disease.
| Study | Total Number of Specimens with Initial Biopsy Diagnosis as MIS | Number Found to have an Invasive Component After Complete Histopathologic Examination of the Lesion | % MIS Upstaged to Malignant Melanoma |
|---|---|---|---|
| Bosbous et al, 2009 | 49 | 6 | 12 |
| Al-Niaimi et al, 2009 | 37 | 5 | 14 |
| Möller et al, 2008 | 49 | 6 | 12 |
| Hazan et al, 2008 | 91 | 15 | 16 |
| Mahoney et al, 2005 | 11 | 2 | 18 |
| Huilgol et al, 2004 | 36 | 24 | 67 |
| Bub et al, 2004 | 58 | 3 | 5 |
| Megahed et al, 2002 | 104 | 30 | 29 |
| Osborne and Hutchinson, 2002 | 89 | 5 | 6 |
| Zalla et al, 2000 | 46 | 3 | 7 |
| Cohen et al, 1998 | 29 | 3 | 10 |
| Somach et al, 1996 | 46 | 9 | 20 |
| Weedon, 1982 | 66 | 8 | 12 |
| Wayte and Helwig, 1968 | 85 | 45 | 53 |
| Total | 796 | 164 | 21 |
The type of histologic analysis of biopsy and excisional specimens may be important as well. Prompted by a patient with a diagnosis of MIS who subsequently developed metastatic disease, Megahed and colleagues recently studied the utility of Melan-A compared with traditional hematoxylin and eosin staining in making a diagnosis of in situ versus invasive melanocytic disease. In 104 cases initially diagnosed as MIS by hematoxylin and eosin staining, an additional 30 (29%) were shown to contain foci of invasive disease when the tissue was examined using Melan-A. In the latter group, 2 patients subsequently developed local recurrences or metastases during an average of 23 months’ follow-up.
Finally, preliminary studies describe how confocal microscopy may help guide physicians in the future to determine where to take sampling biopsies within a given lesion of suspected LM/LMM. Its use, however, is currently limited to research centers, and limitations include size, affordability, and accessibility.
Nonsurgical treatment
Nonsurgical treatment for LM, such as imiquimod and cryotherapy, is a cosmetically appealing option especially in the presence of extensive disease. However, these therapies carry a higher potential for incomplete treatment, and with it, the risk of progression to invasive melanoma. In addition, as already noted, a significant percentage of biopsy-proven MIS lesions already contain foci of invasive disease at the time of initial treatment. Radiation and laser therapy have also been used for LM in patients not amenable to surgical treatment.
Imiquimod is a topical synthetic imidazoquinoline amine that exhibits antiviral and antitumor effects through stimulation of both the innate and cell-mediated immune system by activation of toll-like receptors 7 and 8, which induce transcription factor NF-κB and Th1 cytokines such as interferon-α, interferon-γ, and interleukin-12. Further, imiquimod can induce FasR-mediated apoptosis. It is currently approved by the Food and Drug Administration for treatment of superficial basal cell carcinomas, actinic keratosis, and warts. In 2000, Ahmed and Berth-Jones first reported the use of imiquimod 5% cream as a treatment for LM on the scalp in a patient who refused surgical treatment. Because systemic interferon-α is used for metastatic melanoma, they chose to try imiquimod for its potential to stimulate interferon-α locally. In a review of the literature in 2006, Rajpar and Marsden reported that the overall composite clinical clearance rate for LM treated with topical imiquimod was 88%. However, they noted that many of the case reports and small series presented did not confirm complete histologic clearance of tumor, and follow-up times for the majority of studies were less than 3 years, shorter than the cancer standard of 5 years. In a well-designed study in 2007, Cotter and colleagues treated 40 patients with imiquimod 5% cream 5 times a week for 3 months and followed this with a complete staged excision of the area 2 months later. These investigators found an initial complete clinical response rate of 83% (33/40). However, following complete staged excision of all sites, 2 patients were found to have residual LM and a third was found to have an invasive component. Thus, the actual clearance rate was 75%. In 2009, Powell and colleagues reported results from 48 patients treated with imiquimod 5% cream for 6 weeks and then followed for a mean duration of 49 months. The study showed a 77% (37/49) clinical response rate. Punch biopsies were obtained at 3 months’ follow-up in all clinical responders and no recurrences were found. In the 11 clinical nonresponders, one patient was found to have invasive melanoma following complete excision. Finally, in 2010 Van Meurs and colleagues reported a 44% (4/9) recurrence rate in a small case series of LM treated with imiquimod followed for an average of 31 months.
One of the difficulties with imiquimod therapy for LM is that it can provide a false sense of clinical improvement by removing pigmentation, while in fact the area may still harbor atypical melanocytes or malignancy. These lesions require close histologic monitoring posttreatment for potential recurrence and malignant change. In toto, imiquimod is best considered as a therapy for patients with disease involvement and/or comorbidities that preclude surgical removal and reconstruction.
Nonsurgical treatment
Nonsurgical treatment for LM, such as imiquimod and cryotherapy, is a cosmetically appealing option especially in the presence of extensive disease. However, these therapies carry a higher potential for incomplete treatment, and with it, the risk of progression to invasive melanoma. In addition, as already noted, a significant percentage of biopsy-proven MIS lesions already contain foci of invasive disease at the time of initial treatment. Radiation and laser therapy have also been used for LM in patients not amenable to surgical treatment.
Imiquimod is a topical synthetic imidazoquinoline amine that exhibits antiviral and antitumor effects through stimulation of both the innate and cell-mediated immune system by activation of toll-like receptors 7 and 8, which induce transcription factor NF-κB and Th1 cytokines such as interferon-α, interferon-γ, and interleukin-12. Further, imiquimod can induce FasR-mediated apoptosis. It is currently approved by the Food and Drug Administration for treatment of superficial basal cell carcinomas, actinic keratosis, and warts. In 2000, Ahmed and Berth-Jones first reported the use of imiquimod 5% cream as a treatment for LM on the scalp in a patient who refused surgical treatment. Because systemic interferon-α is used for metastatic melanoma, they chose to try imiquimod for its potential to stimulate interferon-α locally. In a review of the literature in 2006, Rajpar and Marsden reported that the overall composite clinical clearance rate for LM treated with topical imiquimod was 88%. However, they noted that many of the case reports and small series presented did not confirm complete histologic clearance of tumor, and follow-up times for the majority of studies were less than 3 years, shorter than the cancer standard of 5 years. In a well-designed study in 2007, Cotter and colleagues treated 40 patients with imiquimod 5% cream 5 times a week for 3 months and followed this with a complete staged excision of the area 2 months later. These investigators found an initial complete clinical response rate of 83% (33/40). However, following complete staged excision of all sites, 2 patients were found to have residual LM and a third was found to have an invasive component. Thus, the actual clearance rate was 75%. In 2009, Powell and colleagues reported results from 48 patients treated with imiquimod 5% cream for 6 weeks and then followed for a mean duration of 49 months. The study showed a 77% (37/49) clinical response rate. Punch biopsies were obtained at 3 months’ follow-up in all clinical responders and no recurrences were found. In the 11 clinical nonresponders, one patient was found to have invasive melanoma following complete excision. Finally, in 2010 Van Meurs and colleagues reported a 44% (4/9) recurrence rate in a small case series of LM treated with imiquimod followed for an average of 31 months.
One of the difficulties with imiquimod therapy for LM is that it can provide a false sense of clinical improvement by removing pigmentation, while in fact the area may still harbor atypical melanocytes or malignancy. These lesions require close histologic monitoring posttreatment for potential recurrence and malignant change. In toto, imiquimod is best considered as a therapy for patients with disease involvement and/or comorbidities that preclude surgical removal and reconstruction.
Excisional surgery
Surgical excision with 5-mm margins around the clinically visible lesion is the current “standard of care” treatment recommendation for MIS. It was established by a National Institutes of Health consensus conference in 1992. Soon afterwards, however, data begin to show a need for wider margins to achieve complete clearance in selected cases, especially with larger diameter lesions and those of the LM subtype located in the head and neck area. In 1994, Robinson reported that a 6-mm margin cleared only 23% of MIS cases and that the recurrence rate after 8 years was 6% (1/16). In 1997, Zitelli and colleagues showed that 9-mm margins were required to clear 95% of MIS cases during Mohs surgery. Based on their data, the investigators recommended the following margins for traditional excisional surgery: 1-cm margins for lesions smaller than 2 cm in diameter located on the trunk and 1.5-cm margins for lesions larger than 2 cm in diameter on the trunk and those located on the head and neck. Zalla and colleagues confirmed these findings and noted that 1.5-cm margins cleared 96% of MIS located primarily on the head and neck. Finally, in 2008 Hazan and colleagues analyzed 117 cases, and again noted a correlation between lesion diameter and the surgical margin necessary for tumor clearance. In a recent review of the literature, 3- to 5-year recurrence rates following surgical excision with 5-mm margins are in the range of 6% to 20%. In about half of these instances the pathology will return with positive margins. Thus, the National Comprehensive Cancer Network guidelines of care for melanoma currently recommend a 5-mm excisional margin for MIS, but a footnote states: “For large melanoma in situ, lentigo maligna type, surgical margins >0.5 cm may be necessary to achieve histologically negative margins; techniques for more exhaustive histologic assessment of margins should be considered.” Therefore, when MIS is being surgically excised, consideration of the lesion’s subtype, location, and diameter can help a surgeon to decide if margins greater than 0.5 cm may be necessary.
The discovery of positive margins on permanent section assessment a week after a surgical excision can be anxiety provoking for many patients, especially if multiple reexcisions are subsequently needed to clear the MIS. When performing a reexcision the location of the positive margin is usually unknown, and therefore an additional layer is often taken from all sides of the lesion, usually around a linear scar. Subclinical spread is usually the reason for the initial incomplete excision, and reexcision is performed without a clear picture of the borders. This situation occurs more often than not because of the ill-defined nature of LM. Furthermore, these lesions occur frequently on cosmetically sensitive areas such as the head and neck, where a tissue-sparing technique would be valuable to both maximize cure rate and minimize final defect size.
Mohs Micrographic Surgery
MMS achieves the goals of maximizing cure rate and minimizing defect size by employing CPME during excision. Although challenges exist in interpreting frozen sections of melanocytes, the literature indicates that MMS is a successful therapy for LM, with much lower recurrence rates than nonsurgical methods and standard 5-mm margin surgical excisions ( Table 2 ). There is a range of MIS recurrences rates after MMS, and it is likely an operator-dependent and technique-dependent process ( Table 3 ). Several forms of CPME are described in the literature for LM including traditional frozen sections, frozen sections with a final layer sent for permanent sections, frozen sections with immunostaining, and staged excision with rush permanent sections.
Related posts:
 Mohs Micrographic Surgery Technique
Mohs Micrographic Surgery Technique
 Mohs Surgery for Squamous Cell Carcinoma
Mohs Surgery for Squamous Cell Carcinoma
 Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
 Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


