Microcystic adnexal carcinoma is a rare neoplasm with a propensity for slow growth and extensive local invasion. Pathology is characterized by multiple islands of basaloid epithelial cells, ductal structures, and keratinizing cysts, located intradermally but often extending deep as thin strands of tumor cells intercalating between collagen bundles. Perineural and intramuscular invasion are common. Treatment with Mohs surgery allows for fewer procedures with increased likelihood of long-term cure and tissue conservation.
Microcystic adnexal carcinoma (MAC), also known as sclerosing sweat duct carcinoma , malignant syringoma , and syringoid carcinoma , was first described as a distinct clinicopathologic entity in 1982. MAC is a tumor with follicular and sweat gland differentiation and overall benign features histologically; however, it exhibits aggressive local behavior. This article describes clinical presentation, pathologic hallmarks, and treatment options.
Clinical presentation
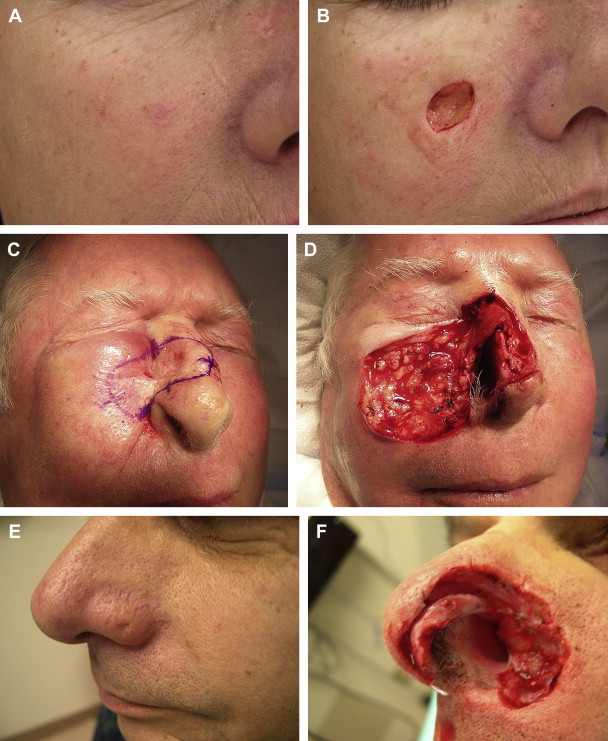
MAC is an uncommon tumor. In a retrospective case series at a Mohs referral center, the mean number of cases per year was 1.63. MAC generally presents a smooth flesh-colored or yellow slow-growing indurated plaque or cystic nodule on the central facial region ( Fig. 1 ). The average tumor size at diagnosis is 2 cm. Other rare locations include the scalp, axillae, buttocks, and genitals.
Surveillance, Epidemiology and End Results (SEER) database analysis of 223 patients showed middle-aged to older patients are preferentially affected (median age, 68 years), and the most common site of involvement is the head and neck, including the lips (74%). MAC rarely occurs in children. Women were affected more often than men (57% vs 43%). MAC was noted mostly in whites (90%). A cases have been reported in African Americans, and in Japanese, Puerto Rican, Korean, Spanish, and Jewish people. Similar demographics were described in a large case series from University of California, San Francisco (UCSF). This series also reported left-sided predominance. Another smaller series of patients with MAC referred for Mohs surgery also described 6 of 10 cases occurring on the left side. These investigators postulate a possible role of ultraviolet light in the pathogenesis of this tumor. Radiation may increase the risk of developing MAC. Three cases have been associated with immune suppression: two in renal organ transplant recipients (one who also had radiation for acne) and one associated with chronic lymphocytic leukemia.
MAC is slow-growing but can be locally aggressive. Generally, the extent of tumor burden is confined to the skin (in 75% of cases according to the SEER database). However, invasion into underlying soft tissue, muscle, and bone is possible. In fact, because of subtle clinical presentation, MAC is often diagnosed at a later stage and has invaded deep into the dermis or subcutis by diagnosis. One case report describes a patient who presented with an indurated plaque over the chin and was found to have tumor invading the mandibular bone marrow.
MAC is usually asymptomatic, but if perineural involvement is present, patients may report or complain of numbness, paresthesia, or tingling. Yu and colleagues noted lymph node involvement in 1% of patients, and only 1 case in 223 was metastatic. Although MAC causes high morbidity because of its locally aggressive nature, overall survival is good, and death secondary to MAC is unlikely. Yu and colleagues note a 97% 10-year survival rate, which is similar to patients of similar age without MAC.
Clinical differential diagnosis includes benignadnexal tumors, such as trichoepithelioma, trichoadenoma, and syringoma, and a scar, cyst, basal cell carcinoma (especially the morpheaform subtype), and squamous cell carcinoma.
Histopathology
On initial description, microcystic adnexal carcinoma was believed to originate from an adnexal keratinocyte capable of undergoing follicular or sweat gland differentiation. More recently, cases of MAC have been reported with sebaceous or apocrine differentiation. Most authors agree that MAC has follicular and eccrine origins.
Pathology is characterized by multiple islands of basaloid epithelial cells, ductal structures, and keratinizing cysts, located intradermally but often extending deep as thin strands of tumor cells intercalating between collagen bundles. Stroma is often fibrotic, and perineural and intramuscular invasion are common. The tumor is not well defined. Tumor cells often appear benign with lack of cytologic atypia, and few if any mitoses.
Histopathologic analysis is necessary for diagnosis. Tissue biopsy must be of adequate depth and size because architectural features are important in diagnosis. In one case series, misdiagnosis occurred in 27% of cases. In another prospective study, MAC was diagnosed intraoperatively during Mohs surgery in 32.5% of cases (these patients had been referred for excision of a different lesion). Often misdiagnosis is secondary to inadequate sampling, because the pathologist cannot see the breadth or depth of the tumor. Also, the bland histologic features with little cytologic atypia or mitoses can make diagnosis difficult.
Differential diagnosis on histopathology is similar to the clinical differential diagnosis, and includes morpheaform basal cell carcinoma, desmoplastic trichoepithelioma, syringoma, and trichoadenoma. Ductal features differentiate MAC from desmoplastic trichoepithelioma and trichoadenoma. Asymmetry, single-cell strands, and perineural and intramuscular (deep) invasion differentiate MAC from a syringoma (which tend to be symmetric, circular, and well-circumscribed). Squamous cell carcinoma and metastatic breast carcinoma are also diagnostic considerations.
Immunohistochemistry can help distinguish MAC from other tumors, and highlights eccrine and pilar differentiation. Carcinoembryonic antigen (CEA), epithelial membrane antigen (EMA), and cytokeratin stains are most reliable. Broad-spectrum antikeratin antibodies (AE1/AE3) strongly stain epithelial cells in MAC. EMA stains ductal structures. CEA (which is positive in MAC) helps differentiate microcystic adnexal carcinoma from desmoplastic trichoepithelioma.
Treatment
Surgical modalities are most definitive in the treatment of microcystic adnexal carcinoma. Incompletely excised lesions will recur. Recurrence rates for conventional excision may be as high as 47% (usually within the first 3 years). Mohs micrographic surgery is invaluable for tissue sparing and may increase the chance of cure with fewer procedures. Recurrence rates for Mohs surgery range from 0% to 22% with a 5-year follow-up ( Table 1 ). Currently, most primary tumors are treated with wide local excision (87% of cases in the SEER database), with 10.8% of cases treated with Mohs micrographic surgery. Multiple case series and one prospective study have examined the efficacy of Mohs surgery for treatment of MAC (see Table 1 ).
| Author/Year | Study Type | Number of Cases Treated With Mohs | Primary Vs Recurrent at Time of Referral for Mohs | Number of Recurrences (%) | Average Follow-up |
|---|---|---|---|---|---|
| Friedman et al, 1999 | Retrospective | 11 | 9 vs 2 | 0 (0%) | 5 y |
| Chiller et al, 2000 | Retrospective | 25 | 19 vs 6 | 2 (8%) | 3.2 y |
| Abbate et al, 2003 | Retrospective | 6 | Not specified | 0 (0%) | 23.3 mo |
| Leibovitch et al, 2005 | Prospective | 44 | 30 vs 14 | 1 (5%) | 5 y |
| Thomas et al, 2007 | Retrospective | 25 | 19 vs 6 | 3 (12%) | 39 mo |
| Snow et al, 2001 | Retrospective | 13 | 10 vs 3 | 0 (0%) | 5 y |
| Palamaras et al, 2010 | Retrospective | 9 | 6 vs 3 | 2 (22%) | 5.4 y |
| Hamm et al, 1987 | Retrospective | 3 | 1 vs 2 | 0 (0%) | 19 mo |
| Burns et al, 1994 | Retrospective | 10 | 6 vs 4 | 0 (0%) | 25 mo |
Related posts:
 Mohs Micrographic Surgery Technique
Mohs Micrographic Surgery Technique
 Mohs Surgery for Squamous Cell Carcinoma
Mohs Surgery for Squamous Cell Carcinoma
 Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
Management of Unusual Cutaneous Malignancies: Atypical Fibroxanthoma, Malignant Fibrous Histiocytoma, Sebaceous Carcinoma, Extramammary Paget Disease
 Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Management of Skin Cancer in Solid-organ Transplant Recipients: A Multidisciplinary Approach
Special Considerations for Mohs Micrographic Surgery on the Eyelids, Lips, Genitalia, and Nail Unit
Multidisciplinary Approach to Large Cutaneous Tumors of the Head and Neck
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


