Mohs micrographic surgery (MMS) allows for efficient evaluation of the entire margin in an outpatient setting under local anesthesia with the goal of confirming clear histologic margins prior to reconstruction. The advantages of MMS over standard surgical excisions are multiple: its precise and comprehensive histologic with 100% histologic margin evaluation, higher tumor clearance rates, and maximum preservation of normal tissue. The technique relies on the contiguous nature of most cutaneous tumors. Once serial excision has led to histologic clearance, one can feel confident that a negative margin has been achieved. Further, when Mohs surgery is the chosen method for appropriate indications, 1 the average cost to the patient and the health care system is often less than traditional surgical excisions. 2 MMS has demonstrated 5-year cure rates of basal cell carcinomas (BCCs) to be 99% and 94% for squamous cell carcinomas (SCCs), and offers the highest cure rates for nonmelanoma skin cancers (NMSC). 3, 4, 5
Indications for Mohs Surgery
Recurrent tumors.
Anatomic locations with high rates of recurrence using standard therapies:
Periorbital.
Perinasal.
Periauricular.
Perioral.
Functionally important anatomic locations:
Digits.
Genitalia.
Tumors with aggressive histologic type:
Morpheaform, sclerosing, fibrosing, perineural, metatypical/keratotic, micronodular, infiltrative BCC.
Poorly differentiated, sclerosing, basosquamous, small/single cell, perivascular, spindle cell, pagetoid, infiltrating, clear cell, lymphoepithelial, sarcomatoid SCC.
Perineural invasion.
Size greater than 2 cm in diameter in any anatomic location.
Ill-defined clinical margins.
Tumors arising in scars.
Positive margins on recent excision.
Immunocompromised patients (HIV [human immunodeficiency virus], organ transplantation, hematologic malignancy, pharmacologic immunosuppression).
Genetic syndromes: basal cell nevus syndrome, xeroderma pigmentosum.
Prior radiated skin.
One of the unique aspects of Mohs surgery is that the Mohs surgeon acts as the surgeon as well as the pathologist throughout the entire procedure, allowing a single physician to maintain control and accuracy of tumor extirpation. MMS also offers the maximum amount of normal tissue preservation, therefore optimizing functional and cosmetic outcomes particularly in cosmetically sensitive, functionally important, and/or high-tension areas. MMS is also the preferred method for recurrent or incompletely excised tumors or those that have a high risk of recurrence due to histologic features or due to size in the context of its anatomic location. Larger lesions or lesions in cosmetically sensitive locations that may require significant tissue rearrangement for reconstruction (e.g., flaps or multistaged repairs) should always have clear margins confirmed histologically prior to reconstruction, 6 and MMS is ideal given its rapid and precise approach. While there are clear-cut advantages of MMS, there are also some disadvantages (▶ Table 3.1).
Advantages | Disadvantages |
Local anesthesia used and preferable in patients not amenable to general anesthesia | Requires contiguous tumors |
Tissue preservation in cosmetically or functionally sensitive areas | Improper surgical removal can lead to specimens that are too thick, too thin, or misfolded, leading to decreased pathologic sensitivity |
100% margin evaluation | Poor staining can affect tumor recognition |
Real-time surgery with pathologic evaluation increasing convenience to the patient | Surgeon error in reading histopathology or the procedure itself |
Unable to perform larger cases under local anesthesia |
3.2 History
MMS was developed and pioneered by Dr. Frederic E. Mohs during his tenure at the University of Wisconsin-Madison. Dr. Mohs was studying the potential curative effects of injecting various substances into tumors. During one experiment, he injected 20% zinc chloride solution that inadvertently caused tissue necrosis. Microscopic analysis showed that the tissue retained its structure as if it had been excised and processed for standard histologic assessment. Dr. Mohs realized that this effect of tissue fixation could be paired with surgical excision to remove tumors in a serial manner. He first published his findings in 1941 in the Archives of Surgery where he described treating 440 consecutive patients over 4 years using this technique. 7
His original technique involved the application of zinc chloride paste to the tumor 24 hours prior to surgical excision. For any areas where positive margins remained, zinc chloride paste was again applied to these margins for an additional 24 hours prior to additional tumor extirpation, and the process was repeated until tumor clearance was achieved. Dr. Mohs also conceived the idea of using horizontal frozen sections to evaluate 100% of the tumor margin rather than the traditional vertical sections, which comparatively only examine approximately <0.1% of the total margin. 8 One of the major drawbacks of the zinc chloride was that it caused local tissue necrosis, and the resulting wounds were more challenging to reconstruct. This limitation also led Dr. Mohs to evaluate healing by secondary intention, which he observed was a cosmetically superior option in concave locations.
Today, tissue processing with MMS no longer relies on zinc chloride but rather using a fresh frozen tissue technique, which was also initially performed by Dr. Mohs in 1953. This fresh frozen technique does not cause local tissue destruction, allows for same-day reconstruction, and remains the standard today.
3.3 Preoperative Considerations
Initially, a thorough history and focused skin examination should be conducted along with clinical lymph node assessment. Important factors to evaluate for include the following: implantable cardiac pacemakers and defibrillators that may affect the use of cautery devices, use of blood thinning medications including warfarin, aspirin, clopidogrel, nonsteroidal anti-inflammatory drugs (NSAIDs), and newer anticoagulating agents (e.g. fondaparinux, argatroban, dabigatran, etc.), as well as herbal supplements including garlic, ginkgo, and fish oil. 9 Allergy to local anesthetics, antibiotics, iodine, latex, and tape products should also be reviewed. True allergy to amide anesthetics is rare and most adverse reactions are likely secondary to sensitivity to epinephrine. If a history of lidocaine allergy is elicited, an ester anesthetic such as tetracaine may be substituted. 10 A social history may elicit long-term alcohol consumption or smoking, which may increase intraoperative bleeding risk and poor wound healing respectively. 11
The pathology report of the biopsy should also be reviewed to ensure that MMS is appropriate and indicated for the lesion. Given the uniqueness of skin pathology, ideally the initial biopsy would have been examined microscopically by a dermatopathologist. Patients with large tumors abutting sensitive structures such as the orbit or nose or invasive lesions that feel fixed to underlying structures clinically may benefit from preoperative imaging (e.g., computed tomography [CT], magnetic resonance imaging [MRI], or positron emission tomography [PET] scans) as well as a multidisciplinary approach with consultation of other specialties such as plastic surgery, otolaryngology, ophthalmology, surgical oncology, and radiation oncology.
Historically, antibiotics were routinely prescribed prophylactically for procedures on the lower extremities, groin, or large defects on the lip, ear, skin flaps on the nose, and skin grafts; 12 however, given the overall low risk for infection, there has been a shift away from the routine administration of prophylactic antibiotics in dermatologic surgery. Currently, antibiotic prophylaxis is provided to patients with high-risk cardiac conditions or prosthetic joints at high risk for hematogenous total joint infection. 13, 14, 15 Antibiotics are also prescribed when the surgical site is infected or when the oral mucosa is breached. 13
3.4 Description of Technique
To ensure correct site surgery, the lesion is identified using photographs and landmarks provided by the referring physician as well as the patient. However, it is imperative not to solely rely on the patient’s perception of the lesion given that they often are unsure and/or incorrect. 16 After the site has been confirmed, the tumor borders are examined, and the clinical margin is marked (▶ Fig. 3.1a). The site is then prepped with alcohol and/or antiseptic solution prior to local infiltration of the anesthetic solution (most commonly a mixture of 1% lidocaine and 1:100,000 epinephrine). The anesthetic may be buffered with sodium bicarbonate in a ratio of 1:10 to increase the pH to decrease the pain of injection. 17, 18 Injecting the local anesthetic slowly also helps decrease the stinging sensation.
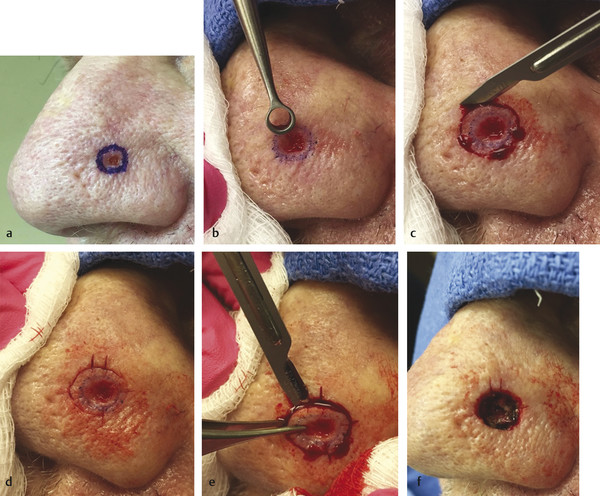
Fig. 3.1 (a) Clinical lesion. (b) Debulking with curette. (c) Periphery of Mohs layer surgically removed with bevel (~ 45-degree angle). (d) Single nicks placed with a no. 15 blade to delineate 3, 6, and 9 o’clock positions and double nicks placed at 12 o’clock position. (e) Base of Mohs layer surgically removed with a no. 15 blade. (f) Defect after first Mohs layer showing nicks at 3, 6, 9 and 12 o’clock positions for orientation purposes. (h) Mohs frozen section showing infiltrative basal cell carcinoma in the depth with its corresponding Mohs map marked with red pencil indicating where the tumor remains.
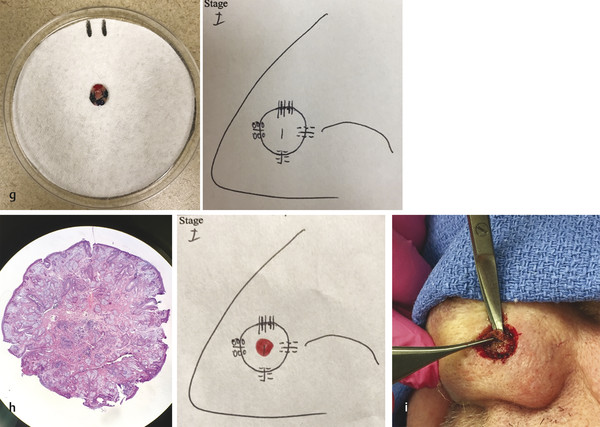
(g) Example of Mohs layer with inking (green ink at 3 o’clock position, blue ink at 6 o’clock position, black ink at 9 o’clock position, and red ink at 12 o’clock position) with corresponding Mohs map with markings representing the colors. (i) Second Mohs layer being surgically removed at the location of positive margins (depth only), preserving as much of the normal surrounding tissue.
The site is then prepped using antiseptic solution, most commonly chlorhexidine or povidone-iodine. After a broad prep, the center of the tumor may be debulked using a curette (▶ Fig. 3.1b), which helps delineate the subclinical boundaries and decrease the number of Mohs layers needed. 19, 20 Some surgeons prefer to perform a sharp debulk of the tumor with their surgical blade, especially for larger tumors. Debulking the tumor also helps for tissue processing to allow for the tissue to flatten appropriately.
After debulking the clinical tumor, the first Mohs “layer” is taken as a disc of tissue with a small margin of normal-appearing tissue around the clinical lesion (▶ Fig. 3.1c). While 1 to 2 mm is the traditional initial margin, the margin may range from 1 to 10 mm depending on the site and the histologic aggressiveness of the primary tumor. Shallow deep margins may be taken on mucosal sites or sites amenable to secondary intent healing. 21 Deeper margins to subcutaneous fat should be taken on other sites. For recurrent tumors, all tissue involved in previous treatments including the entire scar should be surgically removed in the first layer. Infrequently, exceptions of this approach include lesions in anatomic sites where tissue sparing is critical and/or the recurrent tumor is clinically obvious.
For each Mohs layer, the scalpel is held at approximately a 45-degree angle (range of 30–60 degrees) to provide a beveled incision along the entire periphery, which is critical for proper tissue processing. Before removing the deep tissue, the layer as well as the patient’s adjacent normal tissue is marked with superficial nicks (commonly at 3, 6, 9, and 12 o’clock positions) for orientation purposes and tissue mapping (▶ Fig. 3.1d). The deep tissue is then removed with either a scalpel blade or curved iris scissors (▶ Fig. 3.1e) and placed on a piece of blotting paper displaying orientation (▶ Fig. 3.1g). Hemostasis is then achieved with electrocautery (▶ Fig. 3.1f). A sterile pressure dressing is applied and the patient is asked to wait in the waiting room for approximately 1 to 2 hours for tissue processing and any special stains. The surgeon creates a diagram of the excised tissue with its markings to maintain correct orientation (▶ Fig. 3.1g).
To ensure complete histologic assessment of the margins, tissue processing must be executed meticulously. Depending on the size of the lesion, the specimen may need to be cut in multiple pieces to fit on a glass slide. Based on the initial nicks, the specimen’s margins are then inked with different colored dyes to provide accurate pathologic orientation. Consistency in the color coordination helps maintain the correct orientation each time. The goal of MMS is for the surgeon to microscopically assess both the peripheral and the deep margin in a single view. Thus, the tissue must lie perfectly flat so that the epidermis, dermis, and deeper tissues (e.g., subcutis, muscularis, fascia, cartilage, etc.) all lie in a single plane. Extra relaxing cuts may be needed to achieve this goal. 22
The histotechnician subsequently freezes the tissue using a cryostat and embeds the tissue with the deep surface facing up with embedding medium. 23 The frozen sections are then sectioned on a microtome and mounted onto glass slides and stained. The most common stains used for histologic examination are hematoxylin-eosin or toluidine blue, though other immunostains may also be utilized for unique or more aggressive tumors. These frozen sections are then examined by the Mohs surgeon, who assesses whether there is residual tumor at any margin. If tumor remains, the location of residual tumor is marked on the specimen map based on the inking and orientation (▶ Fig. 3.1h).
For additional Mohs layers, the patient is brought back to the operating suite, where the area is again infiltrated with local anesthesia and prepped. Residual tumor in the epidermis and dermis requires extending the periphery of the surgical defect, whereas residual tumor in the deep margin requires removal of the base of the surgical defect (▶ Fig. 3.1i). The surgeon then removes additional tissue only in the area shown to have residual tumor based on the Mohs map while preserving areas that have already been “cleared.” The map, nicks, and inking help orient each layer throughout the procedure. 23 Any tissue removed is again processed by fresh frozen tissue processing in the Mohs lab and examined microscopically by the Mohs surgeon. This process is repeated until a specimen free of tumor is obtained. Once the tumor is removed, the final defect is examined and repair options are explored. Many options exist for management of postsurgical Mohs defects to achieve the optimal functional and cosmetic outcome as will be discussed in subsequent chapters.
3.5 Postoperative Considerations
The postoperative period should take in to account the anatomic location of the defect, patient comorbidities, and the severity and size of the defect. Secondary intention healing often offers cosmetically acceptable results for superficial defects on concave surfaces. 21 Additionally, this approach or a split-thickness skin graft may allow for better tumor surveillance for tumors at high risk for recurrence, whereas flaps or full-thickness skin grafts may “hide” recurrent tumors. Reconstruction often has a shorter healing time compared to secondary intention healing.
Pain control should be addressed postoperatively. While over-the-counter analgesics are often adequate for pain control, oral narcotic agents may be required for opioid-tolerant patients, larger tumors, or wounds in high-tension areas such as the scalp. 24 Patients with NMSC require routine long-term surveillance by their dermatologists as 30 to 50% of these patients will develop another unrelated NMSC during a 5-year follow-up period. 25, 26 These patients are also at an increased risk for developing cutaneous melanoma. 27, 28
3.6 Complications
Patients should be counseled on pain, bleeding, nerve damage, allergic reactions, hematoma formation, infection, necrosis, dehiscence, and scarring during the consenting process. Hemorrhage is a risk both during and after surgery but can be minimized with meticulous hemostasis intraoperatively and pressure bandaging postoperatively. There is no evidence that patients on aspirin or warfarin experience increased risk of major hemorrhagic complications; however, there is an increased risk of bleeding in patients taking clopidogrel or ticlopidine, but these agents are normally continued due to greater risk of thrombotic complications. 29, 30
The most likely artery to be damaged during cutaneous surgery is the superficial temporal artery.
Equally, patients should be counseled on possible nerve injury. Transection of cutaneous sensory nerves are inevitable in skin surgery; however, transection of motor nerves particularly the temporal branch of the facial nerve, marginal mandibular nerve, buccal and zygomatic nerves, and mixed motor and sensory nerves in the posterior triangle of the neck regions may occur as well. 31
Merritt et al in a study of complications after MMS of 1,550 patients showed no major complications including pacemaker or defibrillator malfunction during electrocoagulation. Minor complications were rare as well at 2.6% with active bleeding being most common, followed by infection, necrosis, and hematoma. Further, patients expressed low levels of postoperative pain (1.99 on a 0–10 scale), and 91% reported good control of their postoperative pain. 32 Postoperative infections after Mohs surgery are incredibly low at 0.91%. 33
3.6.1 Nonmelanoma Skin Cancers
NMSC include both BCCs and SCCs, which are the most common cutaneous malignancies, as well as more rare skin tumors. NMSC can be treated with a variety of modalities depending on the histologic diagnosis, size, and anatomic location. Superficial ablative techniques, including electrodessication and curettage (ED&C), and surgical excisions are acceptable techniques for low-risk tumors and produce acceptable cure rates and cosmetic outcomes. For higher risk lesions, more definitive treatment is usually recommended. MMS can meticulously track the deep and superficial invasion of certain tumors, which is the primary benefit and the reason for higher cure rates and lower recurrence rates comparatively. MMS relies on a continuous tumor to fully evaluate the margins and appropriately determine margin negativity. Other incomplete therapies such as topical agents prior to Mohs surgery can create so-called “skip lesions” that can increase rates of recurrence by providing false-negative margins. 34
3.6.2 Basal Cell Carcinoma
Currently, BCCs represent the most common skin cancer. 35 Cure rates of 87 and 95% can be obtained with ED&C and excision, respectively, in low-risk locations such as the trunk and extremities. 35 In a meta-analysis performed by Rowe et al, the 5-year cure rate for a primary BCC treated with Mohs surgery was 99% as compared to 90 to 92% using standard treatments. 3 The 5-year cure rate for recurrent BCCs was 94.4% treated with Mohs surgery compared to 80% for standard treatments. 36 MMS is also preferred for the treatment of large BCCs (defined as 6 mm or greater in high-risk areas/Area H, 10 mm or greater in intermediate-risk areas/Area M, and 20 mm or greater in any area/Area L) given they have a higher likelihood of recurrence and unpredictable margins 37, 38, 39, 40, 41 (▶ Table 3.2). Further, histologic features such as perineural invasion, squamous differentiation, and sclerosis present a high risk for local recurrence, and Mohs surgery is the preferred modality in these instances as well. 42
Area H (high risk) | “Mask area” of face (central face, eyelids, eyebrows, periorbital, nose, cutaneous and vermilion lips, chin, mandible, preauricular and postauricular skin/sulci, temple, ear), genitalia, hands, and feet |
Area M (moderate risk) | Cheeks, forehead, scalp, neck, and pretibial |
Area L (low risk) | Trunk and extremities (excluding nail units and ankles) |
3.6.3 Squamous Cell Carcinoma
MMS is indicated in the management of SCCs with higher risk for recurrence or metastasis including larger size based on anatomic location (defined as 6 mm or greater in high-risk areas/Area H, 10 mm or greater in intermediate-risk areas/Area M, and 20 mm or greater in any area/Area L), recurrent tumors, positive margins from previous excisions, aggressive histologic type such as poor differentiation, as well as SCCs arising within scars. 43 Multiple aggressive SCCs may arise in patients who are immunosuppressed such as solid organ transplant recipients or those with chronic lymphocytic leukemia, and Mohs surgery is preferred in these patients given the high tumor burden and the desire for tissue preservation. 44, 45, 46
Certain anatomic locations represent high-risk sites for SCC recurrence and metastasis including the lips, penis, and ears, or are functionally important such as the hands, and Mohs surgery is preferable in these sites as well. 47, 48 SCC of the mucosal epithelium either on the foreskin, glans penis, or coronal sulcus occurring primarily in uncircumcised men or the labia minora or vestibule in women can also be amendable for Mohs surgery achieving a 5-year cure rate of greater than 90%. 49 Collaboration with a urologist for these genital cases is often helpful.
3.6.4 Melanoma
While the role of Mohs surgery in the treatment of melanoma is becoming more accepted and commonplace, the ability to reliably detect malignant melanocytes in fresh frozen sections had previously been debated. 50, 51, 52 Immunostains such as HMB-45, Mel-5, Melan-A/MART-1, and S-100 increase histologic sensitivity. 53 Recent studies have shown that MMS achieves high cure rates with low risks of recurrence while providing patient convenience of same-day surgery and reconstruction. 54
Proponents of Mohs surgery for melanoma argue that excision with standard margins, especially in head and neck melanomas with extensive surrounding actinic damage, are often inadequate given the extent of subclinical extension of the melanoma. 55, 56, 57 Stigall et al reported 83% of melanoma in situ (MIS) were completely excised with a 6-mm margin, whereas 9-mm margins were necessary to excise 97% of cases, while Felton et al reported 15-mm margins required for a 97% clearance rate. 56, 58 Advocates for using Mohs surgery for melanoma assert that margins needed to clear melanoma can be variable, thus leading to higher rates of incomplete removal of tumors using wide local excision alone. Five-year survival and metastatic rates for 535 patients were the same or better when treated with Mohs surgery than historical controls treated with wide local excision. 59 Alternatively, melanomas may be treated with staged excisions with permanent sections (often dubbed “slow Mohs”) for comprehensive margin evaluation prior to reconstruction. 60, 61, 62 Rapid preparation of permanent sections using microwave technology to create paraffin sections in a few hours rather than 1 day may become more widely used in the future for the treatment of melanomas using the Mohs surgical approach. 63
3.6.5 Other Tumors
Tumors Amenable to Mohs Micrographic Surgery
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


