5 “Simplicity is the ultimate sophistication.” —Leonardo Da Vinci The evolution of procedures for surgical rejuvenation of the face and neck has been progressing since Lexer1 described his technique of undermining and redraping aging facial skin in 1916. Lam2has suggested that Julien Bourguet, several years later, laid the foundation for modern cervical and facial rhytidectomy, noting that Bourguet’s pioneering work in all aspects of facial plastic surgery would reach its fullest expression in his contribution to modern rhytidectomy of October 14, 1919, when Bourguet addressed the Académie de Médecine de Paris to discuss his aesthetic rejuvenation of the neck. In a speech delivered to the same scientific board earlier that year, Dr. Raymond Passot had reported on his more limited technique of rhytidectomy, which extended only from the hairline to the preauricular area. Unlike his contemporary, Bourguet advocated that the incision for the procedure should be carried behind the ear into the hairline, and that extensive undermining should be carried into the neck in combination with a lipectomy—all of which stand as hallmarks of the modern rhytidectomy. Many years passed before 1968, when Tord Skoog3 of Sweden advocated another significant technique, involving elevation of the platysma of the lower face along with the attendant skin flap and advancing that flap posteriorly and laterally when redraping the facial flap. Skoog’s procedure also involved subplatysmal dissection of the cervical platysma. Skoog described the procedure for his rhytidectomy in 1974, before his death in 1975. As reviewed by Lemmon and Hamra,4 who in 1980 reported the first large series of patients treated with Skoog’s technique, the technique provided significant aesthetic improvements in the lower face including the jawline, but the postoperative appearance of the neck and nasolabial fold was not compatible with the improved jawline. Mitz and Peyronie,5 working with Dr. Paul Tessier, reported their work on facial anatomy in 1976, describing in great detail the superficial musculoaponeurotic system (SMAS), which they named after reviewing Skoog’s work. This led to the development of many techniques involving the SMAS, many of which are still in use today. These techniques, whether using imbrications or plication, differ only in the extent of elevation of the SMAS flap or in their direction of vector pull. The net aesthetic improvement with all of the techniques involving the SMAS is a more defined jawline, possibly accompanied by softening of the nasolabial and melolabial folds. As in the subcutaneous rhytidectomy, significant improvement in the appearance of the neck was not seen concurrently, and in the late 1970s various procedures were being developed for contouring of the “unimproved neck.” In 1984 Hamra6 published an article on a new technique that he called “tri-plane rhytidectomy.” Hamra’s triplane rhytidectomy incorporated Skoog’s subplatysmal dissection and wide undermining of the skin in the upper and lower face, but did not continue in the subplatysmal plane in the neck, where his dissection was instead preplatysmal. This technique, still used by Hamra, made it possible to improve the contour of the neck by advancing the cervical platysma muscle anteriorly to some degree and moving the skin and fat posteriorly. Both the medial and lateral approaches to platysmaplasty for rejuvenation of the neck, with or without liposculpture, have many advocates, and are today probably the most commonly used approaches to rejuvenation of the neck. Once again in these procedures, the rejuvenation of the face and that of the neck are seen as distinct operations, and utilize surgical approaches that allow the vectors of pull to differ for the respective rejuvenations of the face, medial neck, and lateral neck. Hamra’s technique continued to evolve to include the deep-plane7 and the composite rhytidectomy.8 My personal technique for rhytidectomy evolved in accord with the techniques just described, and although I did perform several composite rhytidectomies, I found that the technique for this at times affected the function of the orbicularis occuli muscle to a degree that led me to abandon these procedures, and I did not perform composite rhytidectomies after the first year in which I had adopted them as my customary procedures. My preferred technique became the deep-plane rhytidectomy with lateral and medial platysmaplasty to correct concurrent irregularities in the contour of the neck. These techniques indicate that rejuvenation of the aging face and neck has apparently evolved from aesthetic techniques affecting individual compartments and requiring different surgical approaches for optimal surgical correction. For example, several solutions were proposed for improving the appearance of the nasolabial folds through the adaptation of some of the original techniques for this, including the procedures focused on the SMAS and deep-plane and modified deep-plane rhytidectomy. Table 5.1 summarizes the advantages and disadvantages of the various technical variations for rhytidectomy. A different evolution of technique would be needed to achieve optimal rejuvenation of the neck. What if there were a technique that improved the appearance of both the face and neck concurrently and served as the backbone of a procedure for rejuvenating the face and neck? Specifically, is it possible to use a single procedure to address the three most important deformities caused by aging of the face and neck: skin laxity, pronounced nasolabial and melolabial folds, and jowl formation and descent? This definition of the goals of rejuvenation surgery does not fully address periorbital concerns, which usually require some ancillary procedures, but the technique described in this chapter will contribute to softening some aging-related periorbital changes through volume advancement. Table 5.1 Advantages and Disadvantages of the Various Technical Variations of Rhytidectomy
Mixed-Plane Rhytidectomy: The Superior Vertical-Vector Approach to Rejuvenation of the Neck
Facelift Adaptation | Technique and Advantages | Disadvantages |
Subcutaneous | Skin flap created with lateral oblique repositioning. No manipulation of deeper tissues. Uncomplicated and easy to perform | Depending on flap length, does not produce major improvements in aesthetic areas of concern. Results are not durable and may produce a windswept appearance. |
Platysmal flap (Skoog) | Skin flap created with sub-platysmal dissection in the lower face. Lower platysma is repositioned along a lateral oblique vector as a composite unit with the skin flap. Helps to correct jawline contour. Can help correct deformities of neck if performed properly. | More technically difficult to perform and may therefore have more complications. Possibility of lower facial-nerve injury (buccal, mandibular). Misses excessive jowl fat that is more superficial, and produces limited improvement in nasolabial folds. |
SMAS plication/imbrication | Skin flap created. SMAS is plicated, imbricated, or raised as a flap prior to imbrication. Repositioning is along a lateral oblique vector, but some superior vector component is possible. Can be beneficial in all areas of aesthetic concern on the face. Can help correct neck to some degree. | Elevation of flap is time-consuming and sacrifices mechanical advantage by separating flap from deeper tissues. Contour deformities can be visible as a result of removal of tissue from face and neck. Usually requires separate procedures for correcting deformities of the neck. Deeper dissection for SMAS flap elevation usually requires deeper level of anesthesia. |
Deep-plane | Skin flap created with malar fat pad and lower SMAS–platysma integrated as a composite unit. Advantages are similar to those of techniques involving the SMAS, but provides more improvement to the nasolabial folds. Improvement in nasolabial folds increases with subperiosteal elevation of the midface. The skin flap with attached soft-tissue units is advanced obliquely with some vertical component. Temporal hair tuft must be repositioned if a strong vertical component is included in the procedure. Can help somewhat in correcting deformities of the neck | Technically difficult to perform, with more risk of nerve damage and hematoma but less risk to skin flap owing to relative thickness of flap. As with the Skoog rhytidecetomy, persistent fullness of the jowl can result from jowl fat lying in a more superficial plane than that of the the surgical technique. Deep level of anesthesia usually required, and procedure requires long recovery time. |
Composite | Same as deep-plane procedure but includes undermining of orbicularis oculi muscle with lower blepharoplasty. All repositioned units are attached to skin flaps. Same advantages as deep-plane procedure, with added benefit to lax or redundant orbicularis oculi. | Increased risk of nerve injury and hematoma. Deep level of anesthesia is required, and recovery time is long. Dystonias of orbicularis oculi are a real risk. |
Limited-access | Short scar and/or short flap with varying posterior flap development. Plication or pursestring plication sutures in SMAS. Often done with complementary procedures such as fat grafting. Provides good aesthetic improvement with minimal loss of time for patient and minimal risk of complications. Low anesthesia requirements. Moderate correction of neck from vertically oriented plication suture. | Exact placement of plication sutures and tension applied in procedure are not easily appreciated, and variability is possible in side-to-side suture placement. May not be as durable as procedures done with a longer flap. |
Mixed-plane variable access | Dissection in the upper face is similar to that in a deep-plane procedure but more like that in an SMAS plication/imbrication in the lower face. Jowl fat is sculpted and a pure vertical advancement of the SMAS–platysma complex is performed with linear grids. Strongly corrects the neck and all aesthetic concerns, and adds volume to the malar and submalar units. | Volume advancement to the midface yields a very full earlypostoperative appearance in this area of the face. Shortens an elongated face (typical female aging problem), but should be done conservatively in already short or round faces. |
The Surgical Connection of Rejuvenation of the Face and Neck Through a Superior Vertical Vector Approach
The history of facelift surgery is relatively short, and the techniques advocated for it over the past century have been fairly entrenched and until now not very flexible to change. The reason for conservative change in facelift surgery with respect to existing techniques is that the safety of a new technique must be well established in relation to the improvements it may provide in outcome. Moreover, a lasting result must be demonstrated if a new procedure is to be considered “mainstream.” Recently, modifications in technique have been made to simplify techniques for rhytidectomy and make recovery from the procedure easier and the surgery less risky, particularly with reference to risks of anesthesia. Part of this has been driven by patients seeking simpler solutions to facial rejuvenation. In some cases the introduction of less intensive surgical methods is more culturally acceptable if surgery is not the preferred method for aesthetic rejuvenation, as is the case in Europe. As a result of looking for the “holy grail” of surgery that is easy to perform, requires less-intensive anesthesia, and permits a rapid recovery, we are now seeing a burgeoning of innovative approaches to surgical rejuvenation of the face and neck, including endoscopic approaches, limited surgical access, and short-flap surgery that can produce satisfying results in well-selected patients. Table 5.2 summarizes some of the various options for modifying rhytidectomy, as well as a proposed classification for discussing the results of the various techniques for hastening postoperative recovery.
Public demand for rhytidectomy will continue to influence surgical techniques for this operation in the next century to an even greater degree than in the past, as will also the ingenuity of surgeons, which will differ from that in the early and relatively slow development of the procedure. As Tonnard and colleagues9 note in their description of minimal-access cranial suspension (MACS) for facelifting, “Every generation is tempted to speak of? state of the art surgery,? but realistically… there is still much work to be done to achieve the goal of making face-lift patients really look more youthful (and) not just different.” Current thinking, emphasizing volume rather than traction, and vertical vectors rather than oblique or horizontal ones, has advanced the quest for natural facial rejuvenation.
Table 5.2 Gentile Classification of Rhytidectomy
Minilift | Type I (short flap) |
Minilifts are designated as either short-flap or short-scar procedures, including minimal-incision approaches | Flap length from tragus is <3–4 cm Type II (short scar/minimal incision) The incision (s) is limited and does not extend beyond the retrotragal component. A series of small incisions is also classified as constituting a short-scar procedure Type III (combined) Incorporates components of both short-flap and short-scar/minimal-incision procedures |
Intermediate lift | Type I Flap length exceeds 4 cm from tragus Type II Incision extends more than 1 cm into posterior hairline Type III Incorporates both longer flap and longer incision |
Full facelift | Type I-F Incorporates intermediate lift with extended dissection past zygomatic or mandibular cutaneous ligaments or to nasolabial fold Type II-N Incorporates intermediate lift with extended (side-to-side) dissection of neck Type III Incorporates extended dissection of both face and neck |
The use of terms to describe more limited techniques of rhytidectomy or those with more rapid recovery should take into consideration anesthesia requirements, operative time, complication risk, and recovery time.
Before description of the MACS lift, techniques for “vertical-vector rhytidectomy” were rarely advocated as preferred techniques for producing natural and more youthful results. Nor is vertical-vector rhytidectomy compared with the oblique or lateral vector pull that is usually associated with SMAS lifts and to a lesser extent with deep-plane rhytidectomy. The concept of rhytidectomy with a more vertical vector appears to have begun with the S-lift as described by Zaylan.10 We are now seeing greater acceptance of the soundness of the vertical approach with its adaptation by various surgeons. Little11 has also emphasized the importance of vertical-vector techniques, and as those who have utilized a more significant vertical vector in facelift surgery have observed, adequate elevation of the SMAS by plication, imbrication, or suture techniques in the mid- to lower face will also to a large degree correct deformities in the neck. Why is this? This chapter will demonstrate both anatomically and clinically that pulling of the undissected SMAS along a superior vector also pulls the platysma superiorly, through its attachments and tissue integration with the SMAS, and that this has a dramatic effect on the jawline, neck, and chin.
Current Techniques for Facial Rejuvenation via Rhytidectomy
As noted in the discussion of the brief evolutionary history of techniques for rhytidectomy, numerous adaptations of these techniques have been described, with each adaptation carrying risks and benefits, as well as having proponents and detractors. Although nearly all of the conventionally accepted techniques for rhytidectomy achieve the removal of lax or redundant skin, the variations in the approach to the deeper soft tissues distinguish the main differences in these techniques. Recently, limited-incision or short-scar techniques have grown in popularity, but whether a short-scar (incision) or short-flap technique is used, the approach to the deeper soft tissues remains the distinguishing factor in the technical adaptations of rhytidectomy. In most cases the evolutionary flow of technical adaptations in rhytidectomy was driven by the pursuit of more durable, longer lasting, and more aesthetically pleasing results. Recently there has been a more “surgeon-and-consumer driven” de-evolution of technique, and both the quality of the result and the amount of “down time” required to achieve it are now important. Ideally, the best technique for rhytidectomy is the one that produces the best aesthetic result with the least amount of time for patient recovery. The following discussion summarizes most of the conventional techniques for rhytidectomy, with emphasis on the degree of cervical rejuvenation provided by each technique. The techniques discussed are summarized and illustrated in Figure 5.1.
Subcutaneous Rhytidectomy
As noted previously, the initial approach to facial rejuvenation was primarily a subcutaneous approach in which a skin flap was raised by incision between the subdermal layer and the SMAS. The skin flap was advanced, excess skin trimmed, and the flap sutured into its new position (Fig. 5.1A). The redraping in this procedure is predominantly lateral-oblique, and because of the lack of a superior vector the temporal hair tuft is not advanced superiorly. The length of the subcutaneous flap in rhytidectomy when the procedure was initially performed was usually short (<4 cm), but the modifications of subcutaneous rhytidectomy that involve the SMAS are usually performed with a flap ranging from 3 to 4 cm to 6 cm. A consistent anatomical vascular finding in the procedure is the inframalar, midfacial perforating vessel, which is located in association with both the dermal attachments of the parotid masseteric fascia at 4 cm from the tragus (Fig. 5.2A) and the origins of the facial mimetic musculature (zygomaticus major) at ~6 cm from the tragus (Fig. 5.2B).
The main advantages of the subcutaneous rhytidectomy are its uncomplicated nature and ease of performance within a short period, and its lack of a need for deeper planes of anesthesia. The disadvantages of the technique are that it does not produce good short- or long-term results in the areas of the jowl and nasolabial fold, and if done with a limited flap elevation will only tighten the skin somewhat, pulling the lateral skin upward but not correcting the major areas of cosmetic concern. Skin that is stretched excessively and brought up along a lateral oblique vector without adequate undermining can also develop a “windswept” appearance that many patients fear.
Subcutaneous Rhytidectomy: Skoog Modification
The Skoog3 modification of the subcutaneous rhytidectomy (Fig. 5.1B) was the first attempt to improve its aesthetic outcome of the procedure by entry into the deeper soft tissues of the neck. In this adaptation the SMAS–platysma complex in the lower face and neck are undermined and advanced along a lateral oblique vector with a slightly superior component. The main advantage of this technical adaptation of the subcutaneous rhytidectomy was that it provided additional improvements in the contour of the jawline and neck and could be completed with the elevation of a relatively short flap. The disadvantages of the Skoog modification are its potentially additional surgical risk of injury to the buccal and mandibular branches of the facial nerve, and the possibly more stimulating nature of the procedure as the result of its deeper plane of dissection, which may require deeper planes of anesthesia. The aesthetic disadvantage of the Skoog modification is the lack of access to the jowl fat for contouring, owing to the dissection being done in a plane that runs under the masseter muscle and SMAS–platysma complex. In the quest for the ideal rhytidectomy, the Skoog adaptation was also thought to provide inadequate aesthetic improvement to the nasolabial folds, which would leave patients with only a partly more youthful look from the improved appearance of the jawline and neck.
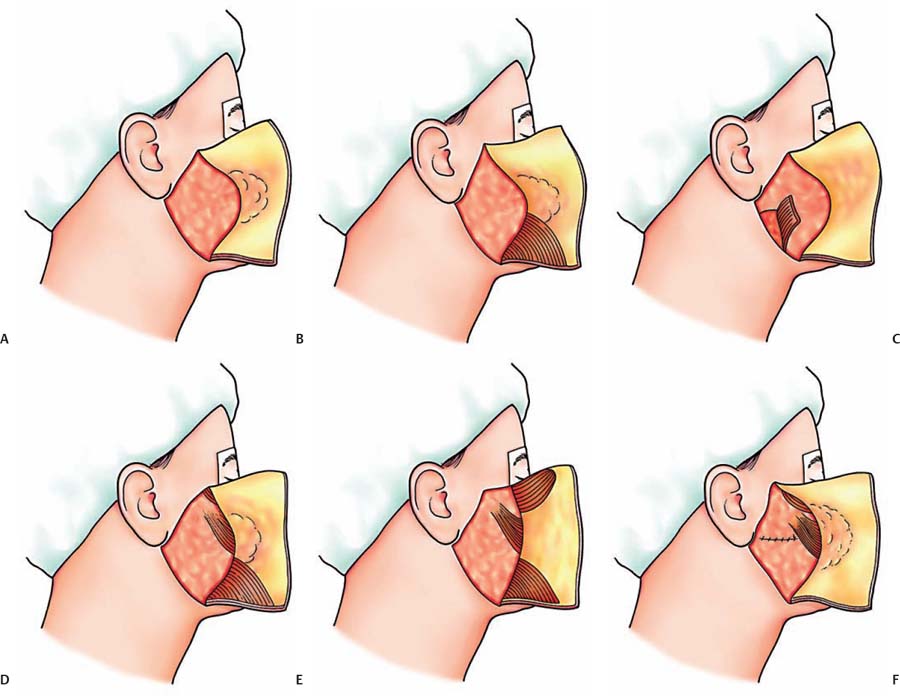
Fig. 5.1 Commonly used techniques of rhytidectomy. (A) Subcutaneous rhytidectomy. (B) Skoog rhytidectomy. (C) SMAS flap variation. (D) Deep-plane rhytidectomy. (E) Composite variation of deep-plane rhytidectomy. (F) Mixed-plane rhytidectomy.
Subcutaneous Rhytidectomy: SMAS Imbrication, Plication, and Excisional Modification
Most of the techniques for subcutaneous rhytidectomy involving the SMAS were developed to enhance its results by providing additional refinements in the jawline, neck, and nasolabial folds through repositioning of the deeper soft tissues of the face. Plication involves a suture technique whereby the deep soft tissue is folded on itself in a manner resembling a pleat in a curtain. Imbrication involves the incision with varying degrees of undermining and subsequent advancement of the deeper soft tissues, followed by their overlapping in a manner similar to the overlapping of tiles on a roof. Excisional techniques involve the excision of a portion of the SMAS and the advancement of associated tissue by suture techniques in such a way that the SMAS can be approximated or imbricated. Excisional techniques are commonly done in a location that will permit softening of the nasolabial folds and enhancement of the contour of the jawline. Most of these techniques involve advancing the soft tissues along a lateral oblique vector of correction. Taken collectively, the techniques for subcutaneous rhytidectomy involving modification of the SMAS add refinements to the cosmetic outcome of the procedure. Many of these techniques can be done without general anesthesia or deep sedation and are both technically easier to perform and shorter than the more complicated SMAS advancement flap techniques. The disadvantages of the excisional techniques are that they can often incompletely correct the appearance of the nasolabial folds. The jowl may also be undercorrected if the flap length is very short. These techniques will usually also not correct the jawline and neck as much as the Skoog and deep-plane modifications of rhytidectomy. For rejuvenation of the neck, other procedures, such as lipoplasty and medial or lateral platysmaplasty, are usually performed concurrently with techniques of subcutaneous rhytidectomy involving the SMAS.
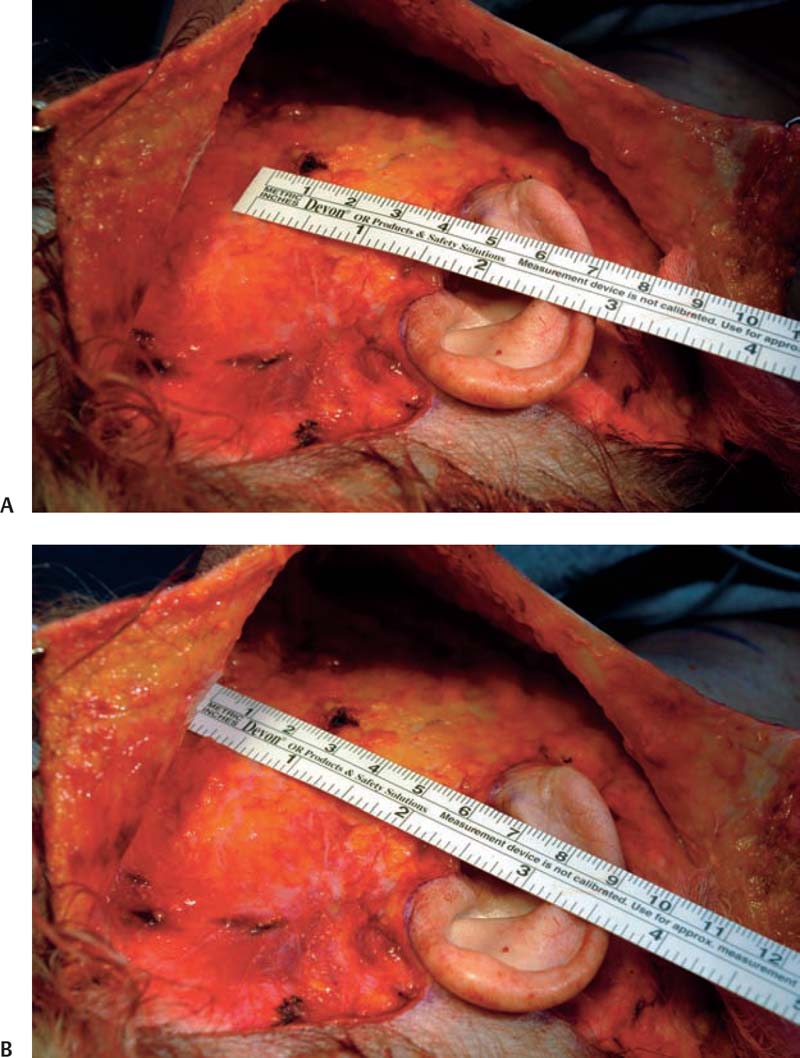
Fig. 5.2 Landmarks in subcutaneous flap elevation. (A) A consistent landmark is the perforating blood vessel in association with the dermal attachments of the parotid masseteric fascia at 4 cm from the tragus. (B) The origin of most of the facial mimetic muscles is at 6 cm from the tragus.
Subcutaneous Rhytidectomy: SMAS Flap Modification
Related posts:
 Preoperative Patient Evaluation
Preoperative Patient Evaluation
 The Aging Neck: Patient Consultation, Physical Findings, and Selection of Rejuvenation Technique
The Aging Neck: Patient Consultation, Physical Findings, and Selection of Rejuvenation Technique
 Direct-Excision Techniques
Direct-Excision Techniques
 Variations in Platysmaplasty: Pursestrings, Slings, and Nonabsorbable and Bioabsorbable Structural Techniques
Variations in Platysmaplasty: Pursestrings, Slings, and Nonabsorbable and Bioabsorbable Structural Techniques
 The Anatomy and Physiology of the Neck
The Anatomy and Physiology of the Neck
 Laser Facial Sculpting, Laser Lipolysis, Smartlifting, and New Technologies for Rejuvenation of the Aging Neck
Laser Facial Sculpting, Laser Lipolysis, Smartlifting, and New Technologies for Rejuvenation of the Aging Neck
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


