Donor site morbidity has become a major focus in free tissue transfer as flap success rates have approached 98%. Emphasis is placed on minimizing the morbidity and optimizing cosmetic and functional outcomes at the donor site. This article reviews techniques to mitigate the donor site morbidity of commonly used free flaps in head and neck reconstruction.
Key points
- •
Donor site morbidity has become a focal point of free flap harvest.
- •
Numerous techniques and adjuncts are described to optimize wound healing at donor site.
- •
Patient education is important to set expectations of donor site morbidity.
Introduction
Free tissue transfer has become the standard for reconstruction of composite large defects within the head and neck. The use of vascularized tissue decreases morbidity and allows for optimal functional outcomes. Free flap survival rates have reached upwards of 98%. The focus has now shifted toward achieving optimal cosmetic and functional outcomes while minimizing morbidity at both donor and recipient sites. This article will focus on the evolution of the management of the donor site.
Many factors contribute to donor site selection. Replacing composite tissue with composite tissue, soft tissue malleability, and limitations of donor sites all contribute to the soft tissue selection, this discussion is outside the scope of this article. We will focus this article on the donor site and its management. The surgeon must carefully weigh the potential donor site morbidity for their specific patient. For example, when considering a composite bony defect an avid runner may be better suited with a scapula or osteocutaneous radial forearm free flap rather than a fibula free flap. Common surgical complications such as wound dehiscence, infection, seroma and hematoma can occur at all donor sites with varying frequency. Table 1 displays specific complications and their incidence for common free flaps used in head and neck reconstruction. Complications are unfortunately inevitable and must be discussed pre-operatively with patients to set appropriate expectations for such complex surgeries.
| Flap Type and Morbidity | Reported Incidence |
|---|---|
| Radial Forearm (RFFF) | |
| Sensory Neuropathy | 1.3–46 |
| STSG Failure (Complete) | 2.7–5.9 |
| STSG Failure (Partial) | 1.8–40 |
| Tendon exposure | 3.5–20 , , |
| Radius Fracture (Osteocutaneous) With prophylactic plating | 0.5–1.9 , |
| Radius Fracture (Osteocutaneous) Without prophylactic plating | 8–67 |
| Decreased Wrist ROM | 16–24 , |
| Anterolateral Thigh (ATL) | |
| Quadriceps Weakness | 4.8 |
| Compartment Syndrome | 0.09 |
| Seroma | 2.4 |
| Muscle Necrosis | 0.09 |
| Lateral Thigh Paresthesia | 24.0 |
| Latissimus/Scapula | |
| Shoulder Weakness | 13–73 |
| Decreased Shoulder ROM | 34 |
| Seroma | 22–79 |
| Rectus Abdominis | |
| Hernia | 0–5 , |
| Umbilical necrosis | 5.4 |
| Fibula | |
| Sensory neuropathy | 6.95 |
| STSG failure | 15–22 |
| Ankle Instability | 4–5.8 , |
| Decreased Ankle ROM | 11.5–12 , |
| Leg Weakness | 8 |
| Foot drop | 1.7 |
| Abnormal gait | 3.9 |
| Compartment syndrome | 0–1 |
This article aims to familiarize surgeons with specific donor site complications and focuses on techniques to minimize the morbidity associated with each donor site in free flap surgery.
Radial forearm free flap
The radial forearm free flap (RFFF) has become one of the most widely used head and neck reconstructive options since its introduction in 1981. As a fasciocutaneous flap with the option to incorporate radius bone as an osteocutaneous flap, it provides a versatile option for the reconstructive surgeon. The anatomy is consistent and straight forward. The soft tissue is malleable and conforms to 3 dimensional reconstructions, while the bony component can be used in limited bony reconstructions. Prior to the evolution of other soft tissue flaps the cosmetic deformity was a minor issue. With the advent of multiple other soft tissue donor sites, the cosmesis of the donor site is often quoted as a limitation to the use of this flap. The presence of a large area of “scar” in a readily visible area can be worrisome to patients. Occasionally, for small defects (typically less than 2 cm in width), the donor site can be closed primarily, which is preferred to minimize this cosmetic deformity. However, the majority of cases require another technique to reconstruct the area. Wound healing complications are common and may lead to prolonged healing with poor cosmetic outcomes. Up to 60% of patients may be dissatisfied with the aesthetic appearance of the donor site, which has led to numerous attempts to find the optimal reconstructive option.
When primary closure is unattainable, surgeons have advocated for local advancement and rearrangement flaps to provide full thickness reconstruction with intact vascular supply. Lane and colleagues described a technique called the “hatchet flap” where the ulnar skin of the forearm is advanced both radially and distally to provide complete coverage of the donor site ( Fig. 1 ). More recently, an ulnar artery perforator-based flap has been described. This technique occasionally requires skin grafting but allows for tendon coverage by the flap with skin grafting over muscle only.

Skin Graft: Split Thickness Skin Graft and Full Thickness Skin Graft
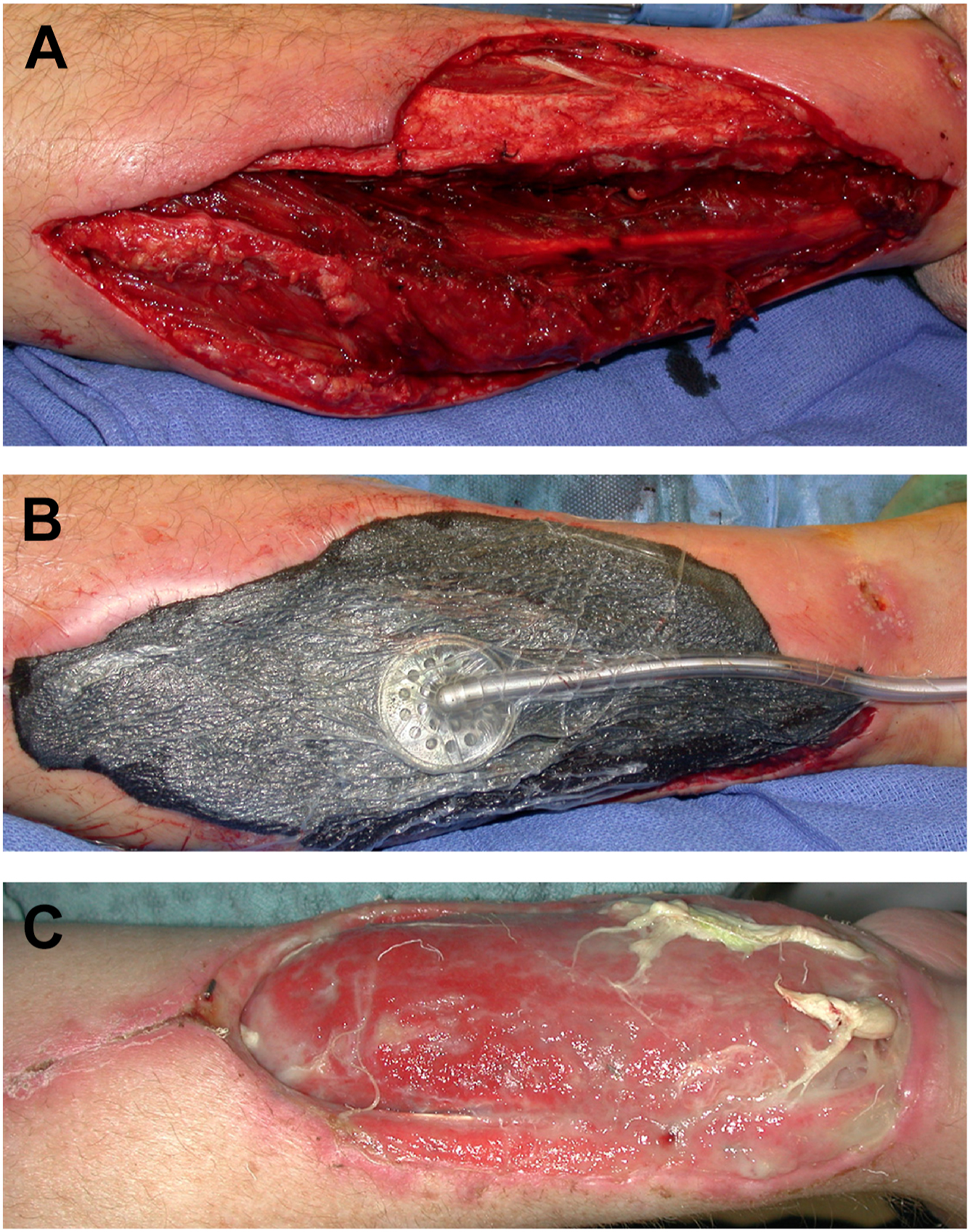
Use of a skin graft: Split thickness skin graft (STSG) has become the most widely used reconstructive technique for RFFF donor sites with varying success rates (see Table 1 ). Skin graft failure can lead to exposure of tendons and delayed wound healing ( Figs. 2 and 3 ); a complication that must be discussed with patients pre-operatively. Additionally, failure to provide tendon coverage can lead to prolonged healing with the possibility of tethering of the tendon to the skin with long-term functional limitations.

A myriad of techniques have been described to mitigate the risk of graft failure and facilitate healing. For skin grafts to be successful, they require a healthy wound bed with good vascularity, adherence of the graft to the underlying tissue, and minimal shearing of the graft over the wound bed. To decrease shear forces at the donor site, bolster dressing along with splinting the donor site has been described. With this technique only 2% of cases have graft failure requiring operative intervention. However, approximately one-third of patients still have partial graft loss with up to 6% experiencing total loss. This leads to prolonged healing of weeks to even months requiring frequent dressing changes by the patient, family, or nursing. Additionally, tethering of the skin and contracture during the healing process after graft loss can lead to functional deficits of the hand and wrist limiting return to full daily activity.
Traditionally harvesting an STSG requires a separate donor site, with additional morbidity. Ghanem and colleagues described STSG harvested from the skin paddle site, eliminating the need for an additional donor site in 97% of cases. However, in elderly or frail patients the surgeon must use caution when employing this technique as it can be challenging to harvest and should consider a separate harvest from the thigh.
Many authors have described a multitude of techniques aiming to augment healing of the STSG, providing better cosmesis and graft take rates. In a prospective study, platelet rich fibrin (PRF) placed in the wound bed increased graft survival rates at the forearm donor site. The use of PRF is thought to improve angiogenesis and fibroblast migration. In a recent meta-analysis, platelet rich plasma decreased graft failure and hematoma formation by 85% and 79%, respectively. The use of Alloderm and acellular dermal matrix has been used as an additional layer deep to the skin graft, which provides improved cosmesis with similar morbidity. , Although these adjuncts may provide improved cosmesis in smaller series, larger randomized studies are needed to truly assess the clinical impact and cost implication of these techniques.
To provide an optimal wound bed and prevent tendon exposure the surgeon should preserve the paratenon over the tendon during flap elevation. Additionally, flexor pollicis longus and flexor digitorum superficialis muscle can be used as a “turn over muscle flap” to provide tendon coverage prior to skin grafting. Authors have also described suprafascial elevation techniques providing fascia coverage to the tendons with improved graft take rates. Additionally, careful attention to detail while securing the STSG will allow for optimal healing.
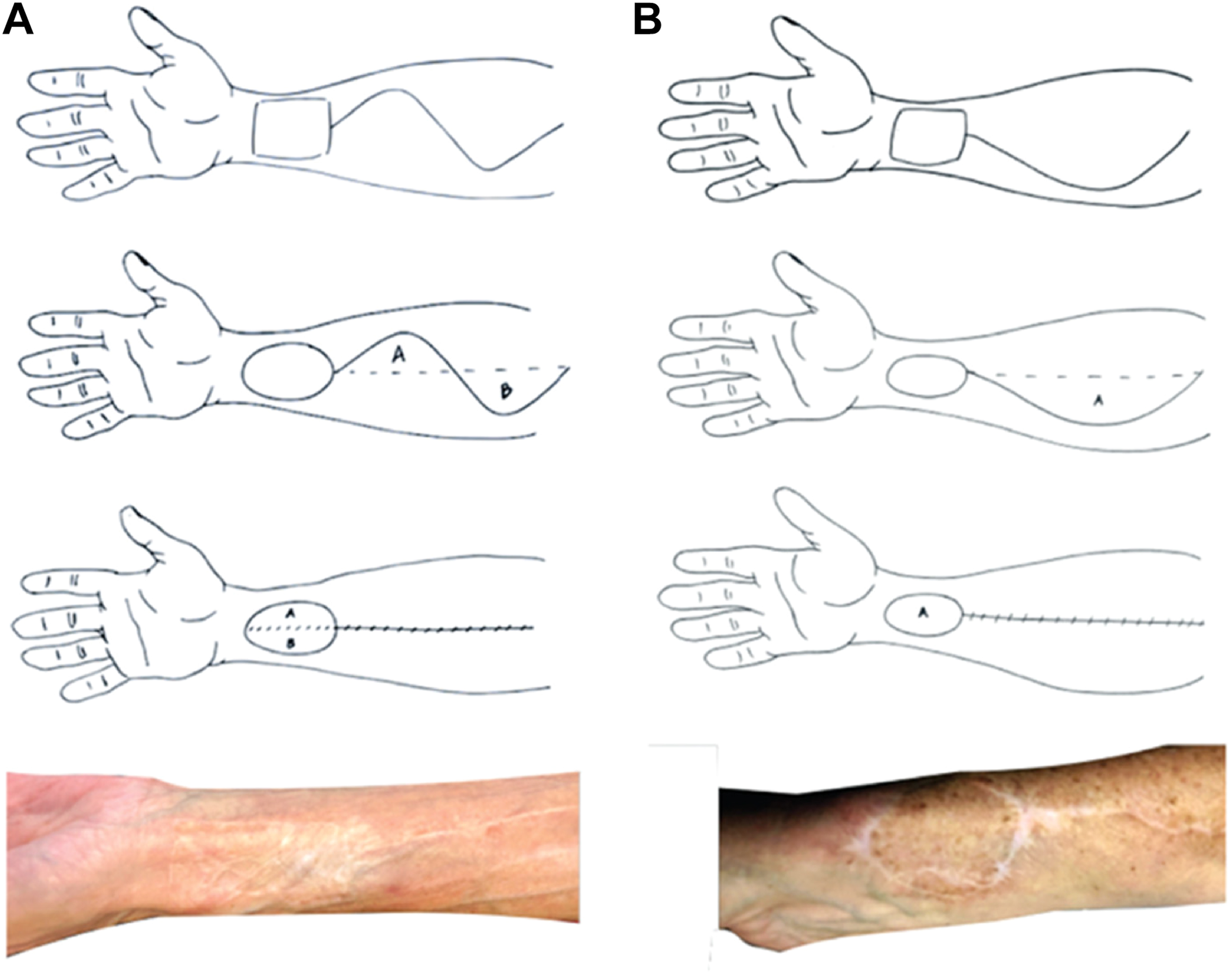
Full thickness skin grafting has been described and popularized due to improved aesthetic outcomes, and elimination of a separate donor site compared with STSG. There is a theoretic decrease in graft take rates for full thickness skin graft (FTSG) due to the thickness of the graft and decreased nutrient diffusion; however, multiple studies have demonstrated similar success rates between STSG and FTSG when used for forearm donor sites. In general, FTSG should be harvested from skin that provides similar color match. Krane and colleagues described a novel technique where an FTSG is harvested from the ipsilateral forearm using a natural curvilinear incision ( Fig. 4 ). This technique requires natural skin redundancy for primary closure of the incision.
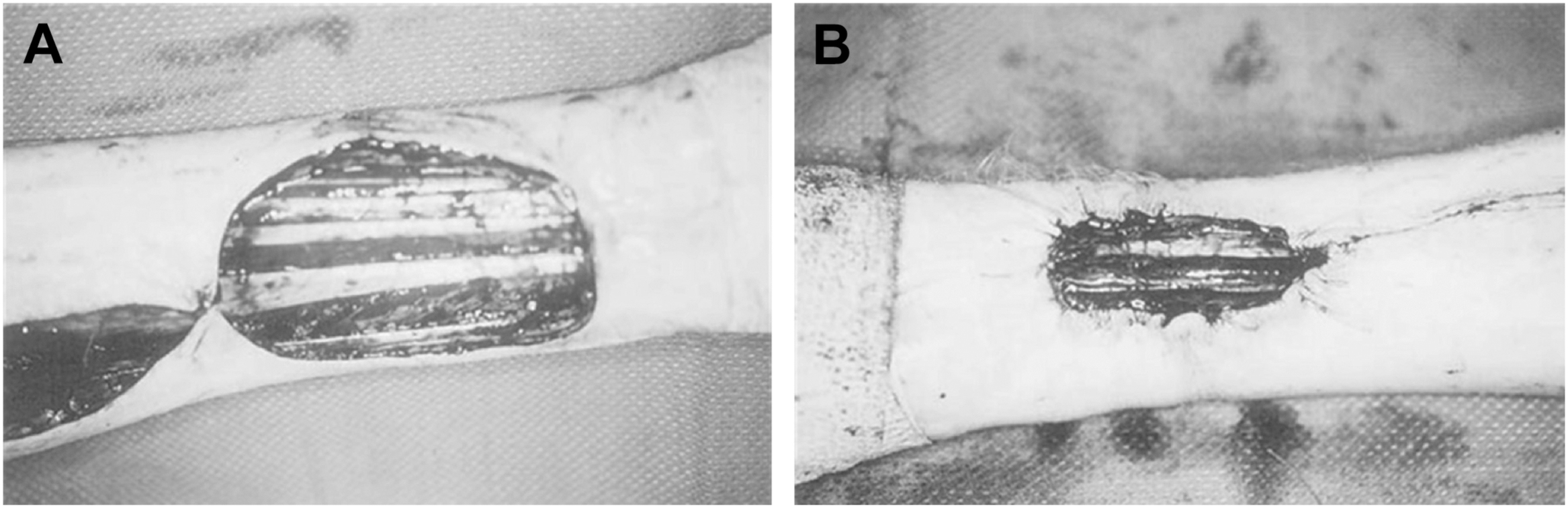
Whether using an STSG or FTSG, smaller defects have lower skin graft failure rates with improved cosmesis. In an attempt to reduce the defect size, Winslow and colleagues described the pursestring technique. By placing a circumferential suture in the dermal layer, the defect size can be reduced by an average of 44.5%. Fig. 5 demonstrates defect reduction with the application of this technique.
Negative Pressure Wound Therapy
The use of negative pressure wound therapy (NPWT) has become increasingly popular in the management of difficult soft tissue wounds. Recently, authors have described the use of NPWT as an adjunct to improve skin graft healing rates. NPWT provides symmetric pressure across the wound allowing for good approximation of the skin graft to the underlying tissue. Additionally, it increases oxygen delivery to the skin graft, which combined with the former suggest an optimal environment for graft success. When compared with traditional dressings in a meta-analysis, NPWT skin graft failure rates were similar. Multiple studies have also demonstrated no statistically significant difference in wound infection, dehiscence, tendon exposure, or need for revision surgery with the use of NPWT. This combined with the cost of NPWT precludes its routine use and should be reserved for wound healing complications at the donor site.
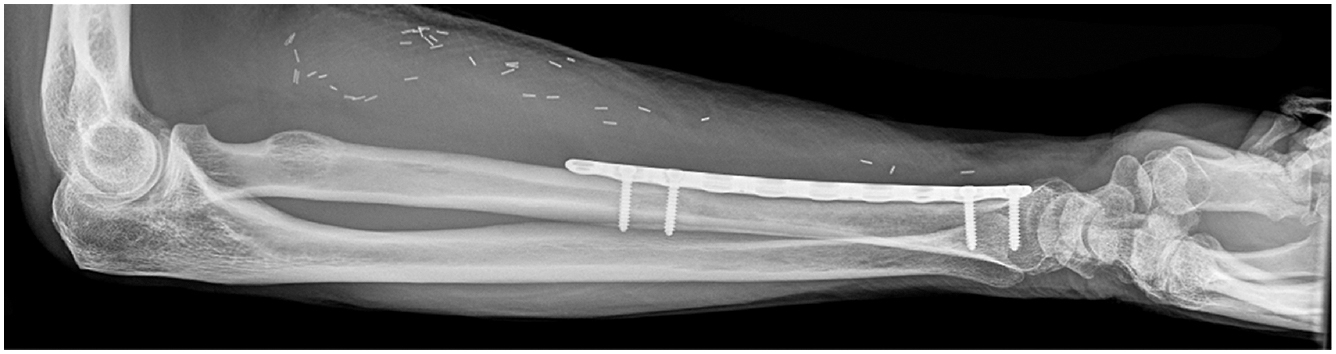
Prophylactic Plating of Radius
Radius fracture has been a feared complication when incorporating bone into an osteocutaneous flap. Initial reports described fracture rates up to 67%. The “boat” shaped harvest with tapered osteotomies rather than traditional 90-degree ostoeotomies was introduced to strengthen the remaining radius. However, cadaveric studies demonstrated similar biomechanical strength for each harvest technique. The use of prophylactic open reduction internal fixation of the radius after harvest was subsequently described ( Fig. 6 ). This combined with boat shaped osteotomies and preservation of 50% to 60% of the radius cross sectional height has led to significant reduction in fracture rates. Periprosthetic fractures are exceedingly rare but have been reported and typically occur distal to the plate. This is a complication the surgeon must be aware of as this is quite debilitating to patients and if recognized and treated early patients can maintain good functional outcomes. Plate exposure can also occur following osteocutaneous radial forearm flap (OCRFF) and is mitigated by using flexor digitorum superficialis muscle to provide plate coverage.