Introduction to Minimally Invasive Scar Management
Despite numerous surgical or energy-based interventions that may be offered to patients with scars, a variety of patient- and scar-related factors may influence the clinician and the patient to choose a less invasive treatment. In this chapter, we discuss minimally invasive scar treatments, including dermabrasion, microneedling, subcision, fillers, and neuromodulators.
Dermabrasion
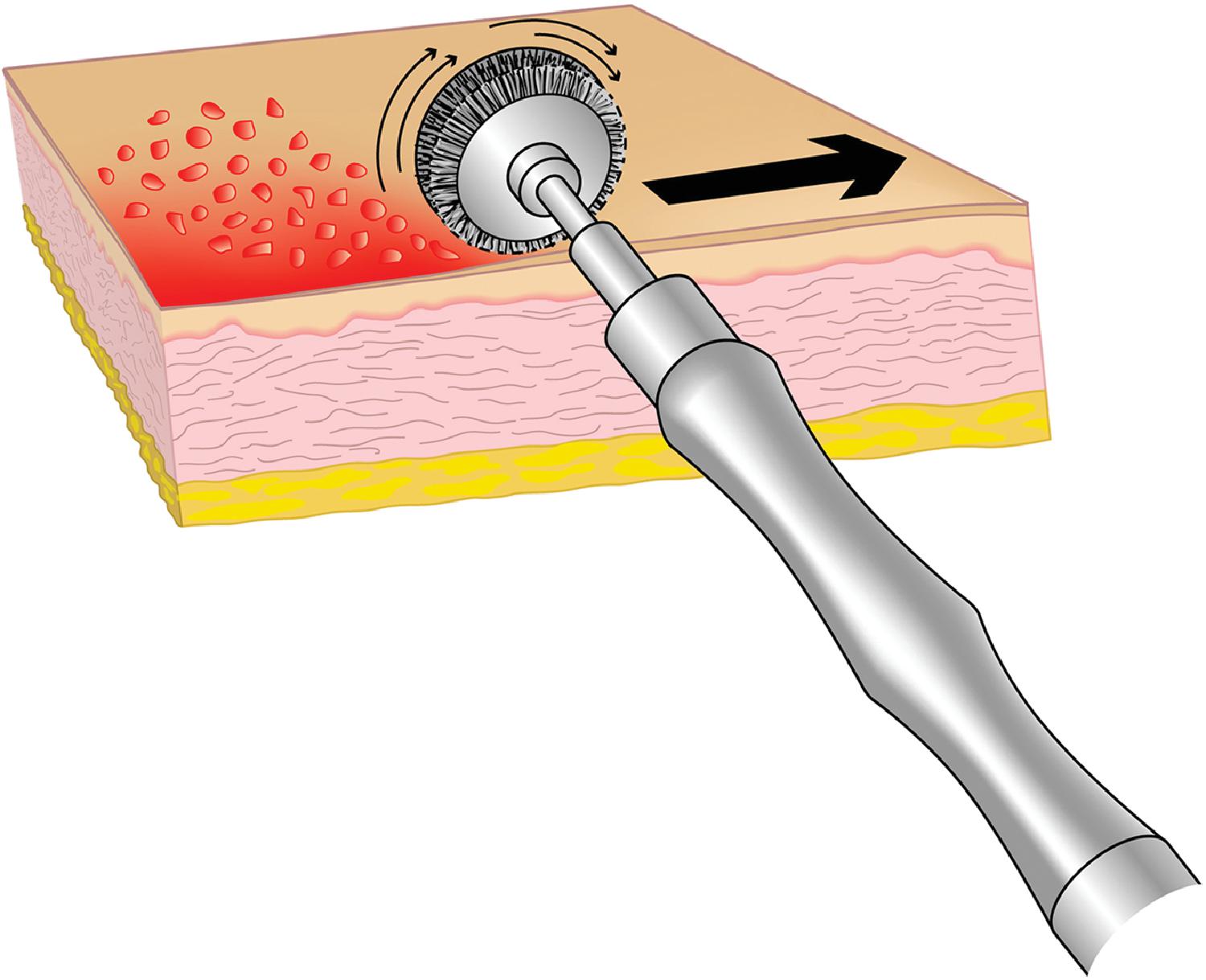
Varying methods of mechanical dermabrasion have been employed since the 1940s as a deep resurfacing technique for the treatment of facial scars. The earliest techniques were developed using sterilized sandpaper and wire brushes. The wire brush essentially consists of a circular instrument with hundreds of thin wire cylinders emanating from the center, with each protruding about 2 mm ( Fig. 4.1 ). The circular piece rotates thousands of times per minute and is applied to the skin surface. In order to prevent the skin from curving under the wire brush surface, the skin is traditionally cooled to the point of freezing with a coolant such as ethyl chloride. This not only anesthetizes the skin but also prevents the wire brush from walking, skipping, and ricocheting.
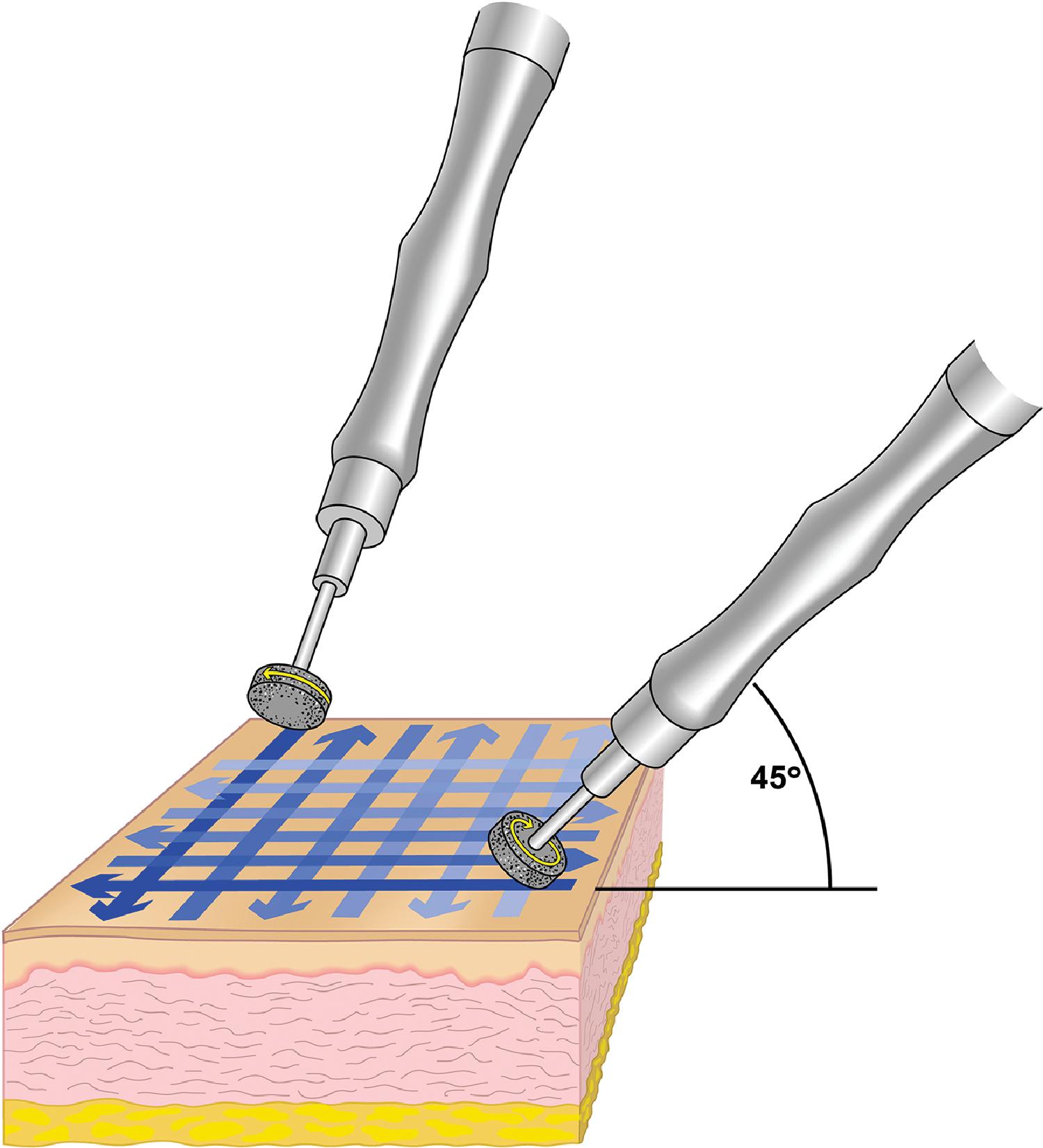
The diamond fraise is relatively newer than the wire brush. Though it, too, employs a rotating circular abradant, it is studded with a thin layer of coarse diamonds as opposed to the emanating wires of the wire brush ( Fig. 4.2 ). This has the advantage of less skin distortion and a more even and predictable dermabrasion than the wire brush. It also allows the surgeon to operate the fraise at a higher rotational frequency (30,000–85,000 rotations per minute) than the wire brush (maximum of 25,000 rotations per minute), which confers greater efficacy.
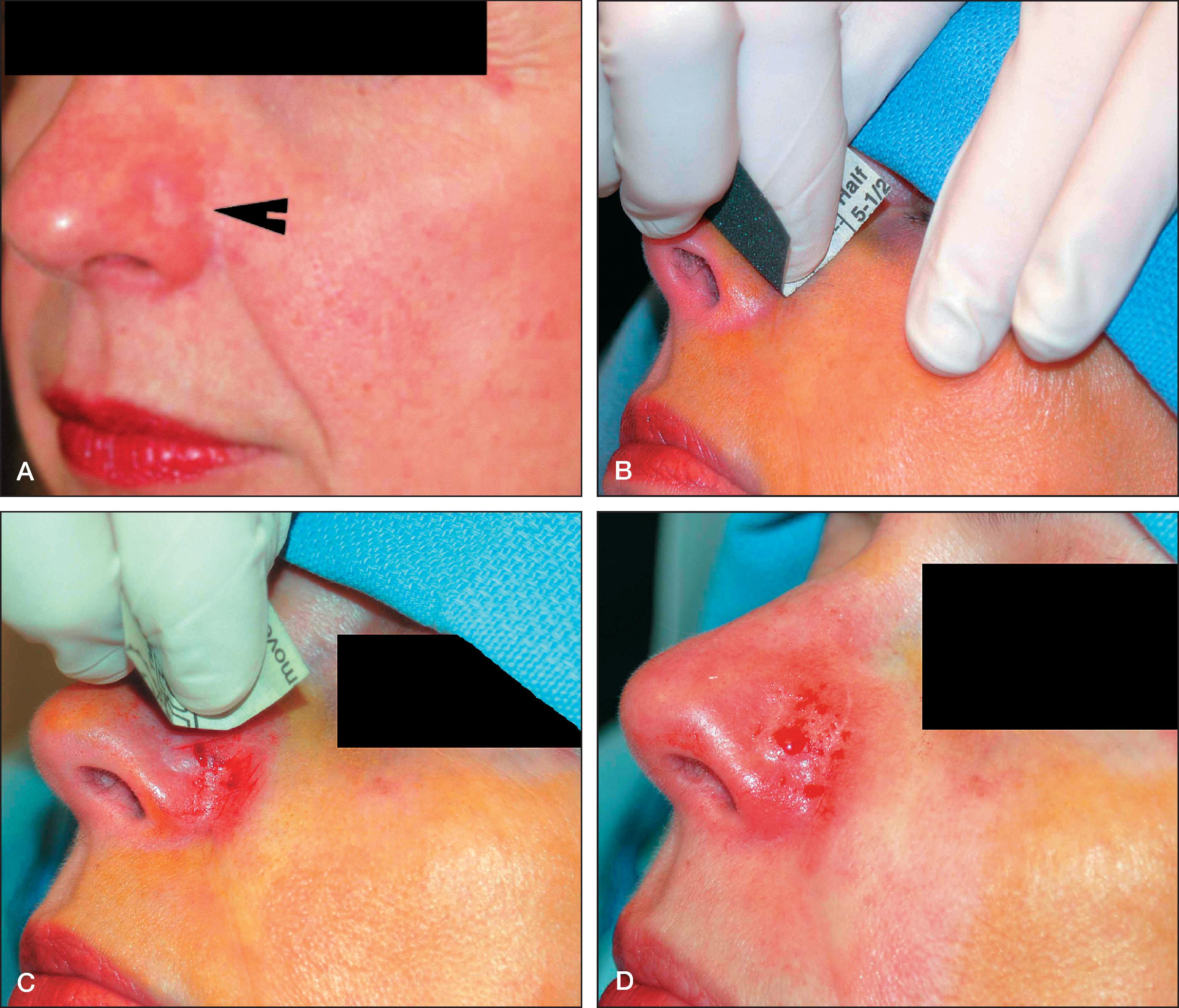
Dermabrasion with sterile sandpaper is a cost‑effective method to achieve similar results as above. It is performed by sterilizing sandpaper (ideally a waterproof brand) and then rubbing the affected area until deepithelialization occurs. In addition to being more accessible and less expensive than wire brush or diamond fraise dermabrasion, it is also more hygienic for the practitioner, as it does not result in blood splatter or aerosolization of the abraded tissue. Outcomes are typically best when used on scars on the face where blood supply is rich. Skin is first cleaned with an antiseptic and then may be anesthetized with lidocaine or an equivalent. Areas that the practitioner does not wish to treat may be covered with adhesive tape. Sanding should generally begin with a coarser-grade sandpaper such as a 200-grade paper and then proceed to finer grades such as a 400-grade paper ( Fig. 4.3 ).
For any method of dermabrasion, hemostasis may be achieved by dripping lidocaine with epinephrine on top of the wound. Depending on the extent of the wound, one may choose to use prophylactic antibiotics, either topical or systemic. Healing typically occurs within 10 to 14 days depending on the extent of the dermabrasion, both in terms of depth and treated area. While resurfacing lasers tend to be more frequently used, the above methods of dermabrasion are tried and true methods, developed over the better part of the last century, which are often more accessible with fewer up-front costs. As with any resurfacing modality, risks include uneven pain, infection, scarring, hyperpigmentation, hypopigmentation, and uneven improvement, and patients must be counseled extensively on these risks prior to the procedure.
Microneedling
Microneedling is a method in which an array of microscopic needles is applied to the skin’s surface to cause zones of dermal injury with minimal epidermal damage, leading to the wound-healing cascade and collagen remodeling. First introduced in 1995 by the Orentreichs as “dermal needling,” it has evolved over the last three decades from tri-beveled hypodermic needles as a form of subcision, to pigment-free tattoo needles, to modern “dermarollers” and automated microneedling pens (“dermapens”). It has been used for numerous applications within dermatology, including scars, rejuvenation and treatment of photoaging, wound healing, androgenetic alopecia, alopecia areata, melasma, and drug delivery. Because of the minimal epidermal damage, it is theoretically safe in all Fitzpatrick skin types.
While microneedling is often used for acne scarring (discussed separately in Chapter 9 ), it may also be used for hypertrophic scars, traumatic and burn scars, and other surgical scars. A variety of microneedling devices or arrangements have been used for different applications. Dermarollers are single-use, rolling, circular spools studded with an array composed of hundreds of microscopic needles typically 0.5 to 3 mm in length and 0.1 to 0.25 mm in diameter. Automated microneedling pens are pen-shaped devices with dozens of microneedles operating with adjustable frequency and depth of penetration in a vibrating, stamp-like pattern. Microneedling may also be used along with radiofrequency, which is discussed in Chapter 5 .
With solid microneedling arrays, once channels have been created, one may apply a variety of solutions to the skin for deeper drug delivery. This may include triamcinolone or 5-fluorouracil solution for scars; minoxidil for hair loss; bimatoprost for hypopigmented scars; or platelet-rich plasma for facial rejuvenation. Additionally, microneedling arrays may be created with hollow needles (through which medication may be applied), with medication-coated microneedles, or with microneedles composed entirely of medication (dissolving microneedles) that themselves create channels and then dissolve into the subsequent wounds.
Subcision
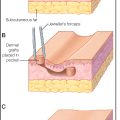
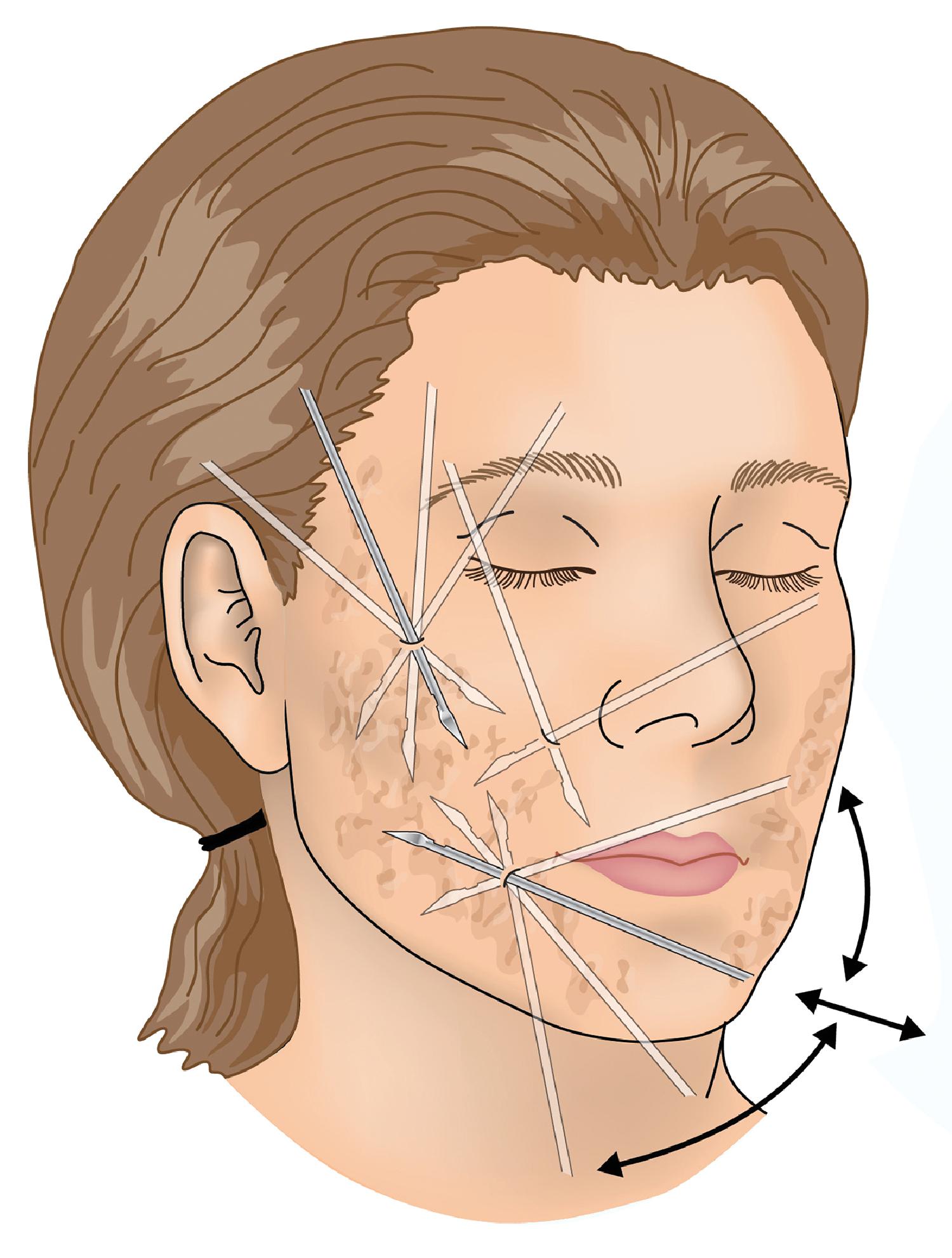
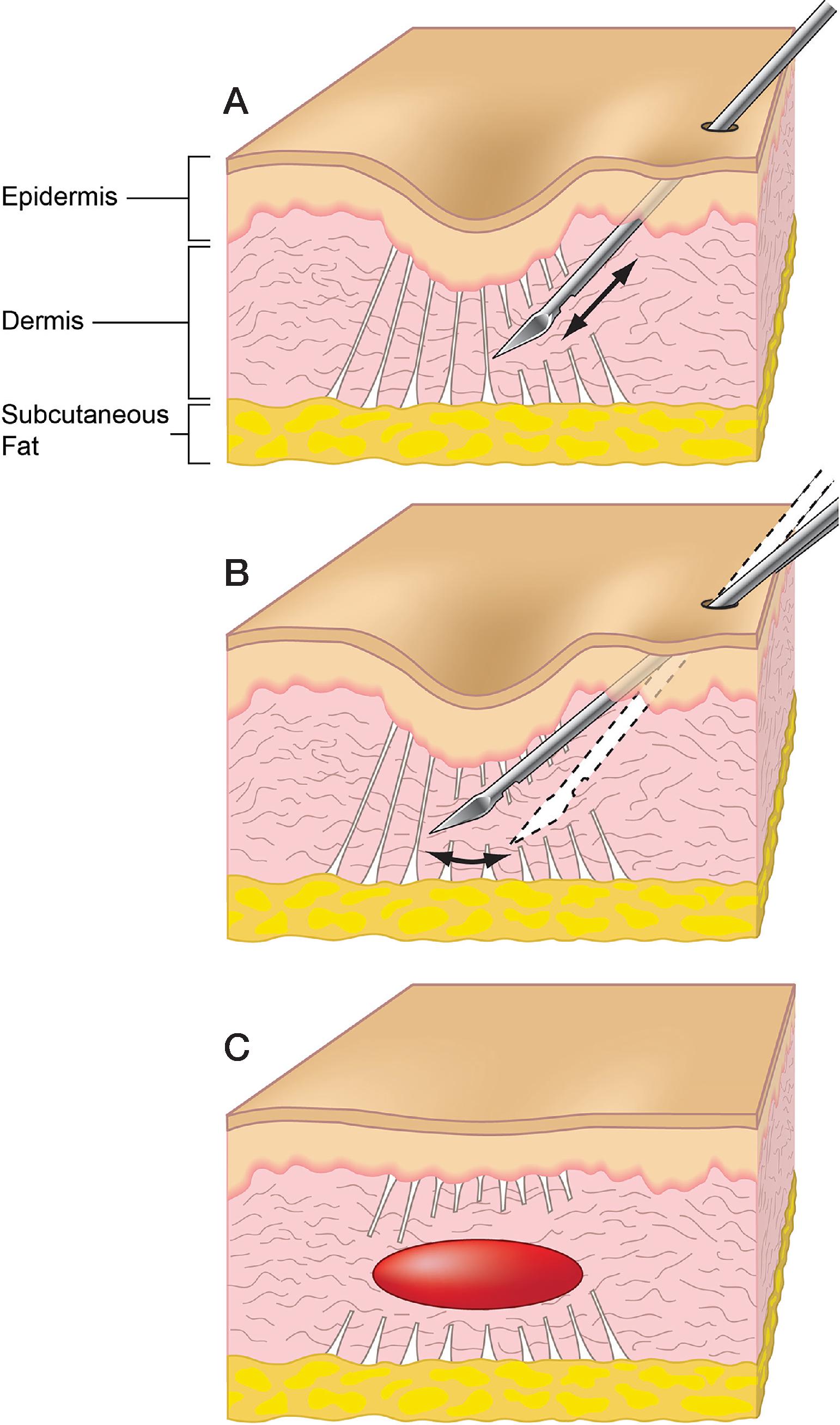
Subcision, also known as subcutaneous incisionless surgery, is the method by which a scar is “untethered” from underlying attachments via the use of a needle, often a specialized cutting needle such as an 18-gauge Nokor needle (Becton Dickinson and Co., Franklin Lakes, NJ). It was first developed by the Orentreichs in 1995 but has since been refined over the last three decades. While subcision is most commonly associated with its use in treating acne scars (further discussed in Chapter 9 ), it may also be used to treat any depressed scar, as well as wrinkles or cellulite ( Fig. 4.4 ). In addition to freeing the scar from underlying attachments, the resulting blood and serosanguinous fluid that pools under the scar after subcision theoretically results in collagen remodeling, which further aids the scar ( Fig. 4.5 ).
Therapeutic pearls to keep in mind when performing subcision include the following:
- 1.
When performing subcision, it is important to first mark the scars prior to infiltration with local anesthesia, as landmarks will often disappear following injection.
- 2.
Anesthesia may need to be placed broader than the area of scarring to allow for painless entry of the needle.
- 3.
One scar may require multiple entry sites for the needle to allow for multiple angles of approach.
- 4.
The subcision needle should be fanned with the bevel parallel to the skin surface to maximize its ability to sweep horizontally through fibrous connections.
- 5.
It can help to use the nondominant hand to hold the skin taut, but care must be taken to avoid needlestick injuries, as the subcision needle can sometimes exit the skin unexpectedly when it passes through a fibrous area.
- 6.
It can be helpful to place the subcision needle on a syringe or grasp it with a needle driver, which serves as the “handle” with which to guide and leverage the needle.
- 7.
For best outcomes, patients should be informed that scars may require repeat subcision treatments at a later date.
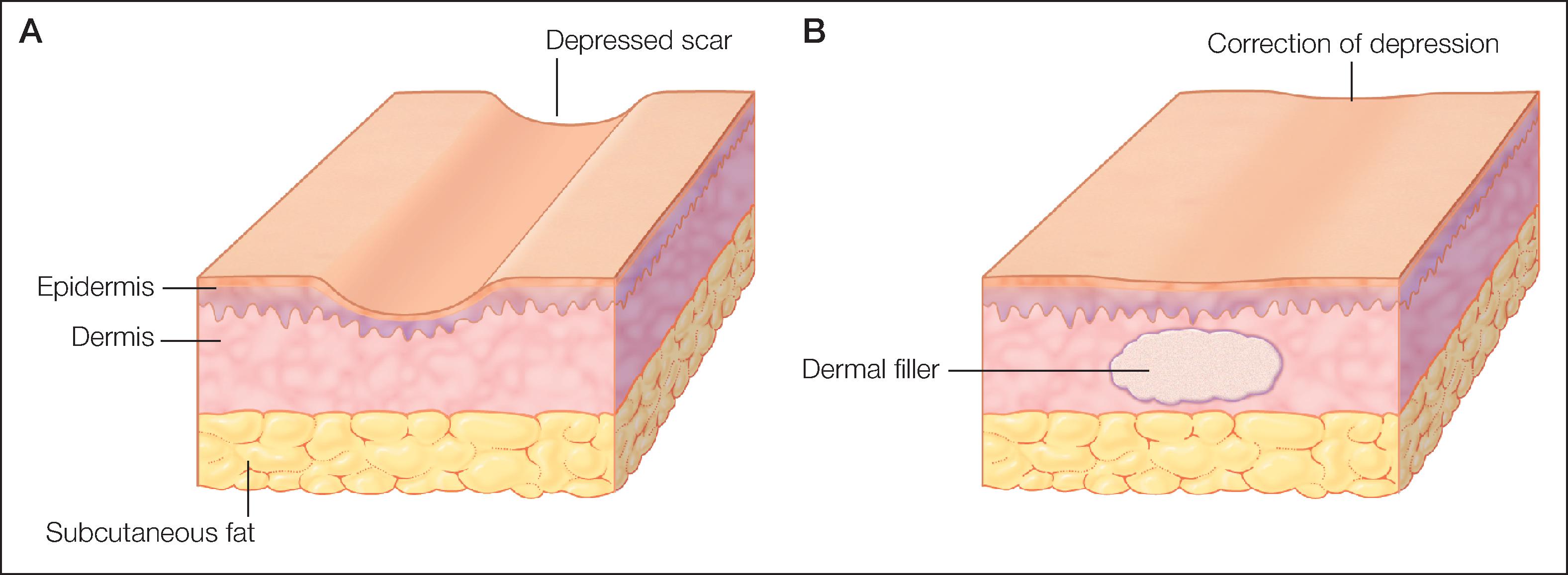
Fillers
For patients with atrophic, depressed scars, fillers are sometimes an option. They also may be performed in combination with subcision once the scar has been “untethered” from any underlying attachments or fibrous cords. Fillers are thought to benefit scars not only by filling volume deficits but also via theoretical biostimulatory effects. The choice of the specific filler generally depends on the area being treated as well as the desired biostimulatory effect (e.g., from calcium hydroxyapatite or poly-L-lactic acid fillers) versus a pure filling effect (e.g., from hyaluronic acid fillers). Each hyaluronic acid filler is manufactured with differing weights, amounts of cross-linking, and complexes, all of which affect the resulting viscosity, density, cohesivity, and other rheological aspects of the filler. Fig. 4.6 depicts the desired placement of filler for scar management. As with subcision, fillers for scars have likely been studied the most with regards to acne scarring, given the depressed nature of the resulting rolling, boxcar, and ice-pick scars; this is discussed in Chapter 9 .