What is the most efficient dissection plane to perform midface lift? What is the best incision/approach (preauricular, transtemporal, transoral)? Why? What specific technique do you use? Why? What is the best method/substance for adding volume to midface lifting? In approaching the midface, how do you see the relationship of blepharoplasty versus fillers versus midface lifting? Analysis: How has your procedure or approach evolved over the past 5 years? What have you learned, first-person experience, in doing this procedure?
Greg Keller, MD with Rahul Seth, MD, Vito C. Quatela, MD with Marcelo B. Antunes, MD, and Jonathan M. Skyes, MD with Christina K. Magill, MD address questions for discussion and debate:
- 1.
What is the most efficient dissection plane to perform midface lift?
- 2.
What is the best incision/approach (preauricular, transtemporal, transoral)? Why?
- 3.
What specific technique do you use? Why?
- 4.
What is the best method/substance for adding volume to midface lifting?
- 5.
- 6.
What is the most efficient dissection plane to perform midface lift?
Keller and seth
The midface lift can be performed in many dissection planes and efficient is a word that has many meanings. So, it depends on what the surgeon wishes to do, how much effort that he/she wishes to expend, what his/her technical capabilities are, what the patient’s signs of aging are, and what sort of result the patient expects.
There are 4 fat pads involved in midface lifting that can be repositioned:
- 1.
Supraperiosteal fat pad, which contributes to the malar crescent and is bound to the periosteum and bone
- 2.
Nasolabial or malar fat pad, which is held up by true ligaments to the malar eminence
- 3.
Buccal fat pad, which is held up by false ligaments
- 4.
Orbital fat, which can bulge anteriorly through the weakened orbital septum and over the orbital rim to the level of the fallen orbicularis retaining ligaments
Descent of these fat pads can be related to gravitational descent, stretching of the ligamentous attachments of these fat pads, and volume loss due to posterior retraction of the malar bone.
In addition, the superficial fascia/superficial musculoaponeurotic system (SMAS), deep fascia, and subcutaneous tissue fuse together and attach to bone at several locations in the midface. These occur at the orbit, the malar eminence, the massateric tendon/malar interface, nasal bone, zygomatic arch, frontal/zygomatic suture lines, etc). There are also ligamentous attachments of the SMAS that progress from bone to the skin of the midface (the malar ligaments, the orbicularis retaining ligament. Sagging of the skin and subcutaneous structures is related to the aging changes in these attachments. Another attachment related to malar edema is the “malar septum” extending from the arcus marginalis to the midface skin.
In addition, volume loss occurs in the face. This is present to a greater degree in the older patient. The skin of the midface is also not immune from the aging process. Both intrinsic and extrinsic causes of skin aging affect the midface.
To obtain a “best” natural appearance, deficiencies of aging related to these pathologies need to be addressed or camouflaged. Aging problems can be multiple and may vary individually or by age group. For instance, a 50 to 60-year-old woman will not have as much volume loss as a 75-year-old woman. Often a “smile test” is helpful to assess volume depletion of the midface. If the patient smiles and the fat pad ascends (meloplication) to fill out the cheek, it is likely that a surgical approach to lift the malar fat pad will work. If the fat pad does not add enough volume with the act of smiling, volume augmentation with filler or implants may be required.
At UCLA, we objectively evaluate our surgical approach based on the patient’s pathology. We have looked at several indicators that help us to do this: the presence of an ogee curve; the distance from eyelashes to the optical bottom of the eyelid; orbital fat protrusion and degree of orbital fat “fall”; anterior projection of the malar eminence, and the presence of a negative or positive vector. While there are other subjective considerations, these indicators are useful in planning an approach. While we favor certain planes and approaches, we may use any or all of the planes that we list below.
For the younger patient, or the surgeon with limited technical capabilities, an “efficient approach” from a surgeon’s perspective, may be to perform a subcutaneous face lift (with or without SMAS plication, such as a MACS or S-lift) and/or inject fat into the cheek to try to camouflage abnormalities. If there is a limited increase in distance from the lashes to the apparent optical bottom of the eyelid, a decent ogee curve, and good anterior projection (all contributing to a “positive vector”), this may produce a happy patient and surgeon (and a short procedure). However, in many individuals, as the edema resolves and the fat disappears, the patient’s preoperative and postoperative photos may not appear much different, except that the jowls and neck are resolved. If the only approach is to camouflage with filler in the setting of significant fallen fat pads, the patient may look artificially bloated (“puffer fish” abnormality) or the cheek may be filled, but the fallen malar pad may still protrude over the nasolabial fold (“rock in the sock” abnormality). In either case, the patient may exhibit an “artificial” appearance.
While many American authors are given credit for sub-SMAS or deep plane procedures, international surgeons are actually responsible for these more sophisticated approaches to the midface. Torg Skoog evolved the deep plane approach to the midface and Tessier, with his fellow, Mitz, explored and evolved the subperiosteal and “low” sub-SMAS procedures. Bosse and Papillon defined the malar retaining ligaments and sub-SMAS procedures to the midface that describe the facial nerve course. The procedures of Bosse and Papillon are, essentially, the “high SMAS” procedures that are used today. I had the privilege of meeting Bosse at an endoscopic meeting and discussing the implications of these procedures on the muscles of facial expression, which are significant and beyond the scope of this discussion. Reading of these authors is essential, should the surgeon wish to perform deeper procedures.
The “low SMAS” procedure involves a limited SMAS dissection plane below the zygomatic arch. Used alone, this approach, by itself, produces little effect on the midface unless it is carried over the malar eminence. It is often used with liporeinjection of the midface. The part of this procedure that is significant for the midface is that, with relaxation and fat reabsorption, a Nike “swoop” line can be produced as, over time, the midface sags over the tightened SMAS. A solution to this problem can be to partially support the midface with a percutaneous “meloplication” procedure of the fat pad or a subperiosteal elevation. For the surgeon with sufficient skill and the patient with a lesser degree of malar sag and shorter eyelid length, this can produce a nice result.
Another set of approach planes to the midface are the deep plane, suprafibromuscular, and “high SMAS” lifts. I group these together, as all of them release the malar ligaments and attachments. A Nike “swoop” line from midface relaxation is usually avoided, but the concavity of the ogee curve can be accentuated. All of these approaches, by freeing up the ligamentous attachments of the midface, allow the malar fat pad to ascend, though this effect may be for a limited time. Combining these approaches with other midface lifting or augmentation techniques can produce a longer lasting result.
Another plane of dissection is the preperiosteal plane of dissection over the malar eminence. This plane of dissection extends under the suborbicularis oculi fat (SOOF) and over the deep fascia of the malar eminence. It is most commonly used from a blepharoplasty approach for orbital fat repositioning. The preperiosteal plane is also a “finger dissection” plane from a lateral and temporal face lift approach over the malar eminence and is used by some surgeons to elevate the malar area during a face lift.
The final plane of approach, and the one that we most often utilize, is the subperiosteal plane. This is the only plane that elevates the malar fat pad, the preperiosteal fat pad, and the SOOF. In addition, the orbicularis muscle, the periosteum and overlying structures adherent to it, and the lip elevators can also be repositioned, if desired. A more extensive description of the technique follows. While a procedure involving a subperiosteal approach is not efficient from the surgeon’s standpoint as it lengthens the procedure time, it is the most efficient approach to reposition fat pads, ligament, and muscle. Tessier described this procedure through a coronal approach and called it a “mask” lift, as it took the “mask” of the fallen face, and restored a youthful appearance ( Fig. 1 ). When I viewed the results of this procedure, I was impressed that the pictures of Tessier, Psillakis and others using this approach were better than any others that I had seen. This procedure was invasive, and we began, in 1989 (procedure patented in 1991), to use an endoscope to reduce the edema associated with it.

Quatela and Antunes
The most efficient plane to elevate the midface is the subperiosteal plane. This plane can be elevated quickly with minimal bleeding. It is also a safe plane to avoid injury to nerves and the facial mimetic musculature. The only nerves that are at risk are the frontal branch of the facial nerve and the maxillary division of the trigeminal nerve. The frontal branch can be avoided if the dissection is performed in the appropriate plane, elevating the periosteum without disruption. The maxillary nerve can be protected by palpation of the foramen and holding pressure at that point while the subperiosteal dissector elevates the midface above and below the exit of this nerve.
Sykes and Magill
In general, the more superficial the dissection plane, the more efficient and secure the lift. Efficiency results from performing only the needed amount of dissection in order to achieve the desired result. In the forehead/brow, for example, the subcutaneous/suprafrontalis muscle dissection plane is more efficient than either the subgaleal or subperiosteal plane. The justification for performing further dissection, using a more distant incision, and developing a thicker flap is to hide the incision and preserve a vascular supply to the flap.
In the midface, the flap needs to be thick enough to camouflage suture irregularities (eg, dimpling), while allowing efficient undermining and elevation of the soft tissue envelope. The possible dissection planes for midface lifting include :
- 1.
Immediate subcutaneous plane
- 2.
Sub-SMAS plane (superficial to the zygomatic musculature)
- 3.
Preperiosteal plane
- 4.
Subperiosteal plane ( Fig. 2 )
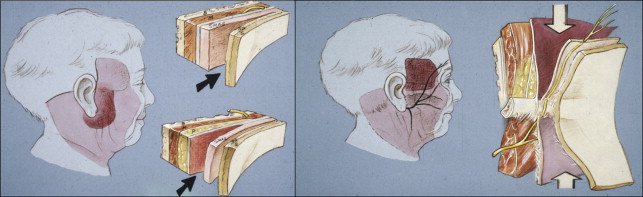
Fig. 2. Sykes and Magill
The tissue layers of the face are shown on the left: skin, subcutaneous issue, the superficial musculoaponeurotic system (SMAS) (investing fascia), the sub-SMAS plane (loose areolar tissue), and parotidomasseteric fascia (deep fascia). The image on the right demonstrates the fascial relationships at the level of the zygomatic arch. The frontal branch of the facial nerve travels in the temporoparietal fascia and is reflected laterally with the overlying subcutaneous tissue and skin. The deep layer of the temporal fascia is beneath the temporoparietal fascia and splits into a superficial layer and a deep layer. The superficial layer of the deep temporal fascia inserts onto the margin of the zygomatic arch and the deep layer of the deep temporal fascia inserts on the medial surface of the zygomatic arch. A fat pad is enveloped between the 2 layers of the deep temporal fascia. Beneath deep temporal fascia lies the deep temporal fat pad the temporalis muscle.
The subcutaneous plane has the greatest chance for contour irregularities, while the subperiosteal plane is the most inefficient, requiring the greatest release of soft tissues. The subcutaneous plane is the most efficient plane for elevation of the midface, but flap fixation can lead to contour irregularities of the facial skin.
What is the best incision/approach (preauricular, transtemporal, transoral)? Why?
Keller and seth
Generally, I prefer a temporal approach posterior to the hairline for lifting the midface. If the temporal incision is placed superior enough (close to the temporal line), an almost vertical direction of pull can be maintained. I will, on occasion, use an extended subciliary eyelid incision, in the face of severe temporal fascia scarring from previous procedures, though I can usually avoid this incision. An extended subciliary incision can produce an eyelid scar that needs to be covered with makeup, and can be associated with eyelid retraction and scleral show.
For positioning of an endotine in the proper position or for placing a malar implant, the intraoral incision is valuable. This incision gives the best access to the lower malar areas and the massateric tendon.
I will often use a transconjunctival incision to retroposition fat over the orbital rim, if orbital fat protrusion is a problem. Often, the orbital fat has protruded through a weakened septum, the globe has recessed, the SOOF fat has fallen, the orbicularis muscle has descended, and the malar fat pad has descended. Overall, this combination of aging effects produces the appearance of a “pot belly over fallen jeans.” This set of anatomic problems can occur even in the younger individual. While all ethnic groups exhibit this “pot belly over fallen jeans” phenomena, many people of Middle Eastern and Asian descent manifest it at a relatively young age.
Quatela and Antunes
Over the course of the years, I have used transoral, transorbital, and transtemporal approaches to achieve midface elevation. In my opinion, the best incision/approach is the transtemporal.
The transtemporal approach, as the name illustrates, achieves midface elevation through a small temporal incision. The dissection starts separating the deep temporal fascia from the deep layer of the superficial fascia and from there to the subperiosteal plane. The forehead and the zygomatic arch are elevated subperiosteally, and this way, as previously mentioned, the frontal branch is protected. The dissection proceeds inferiorly, elevating the soft tissues of the midface from the maxilla. This approach has several advantages over the preauricular and transorbital approaches due to its vector of pull, increased lower lid support, and avoidance of lower lid malposition. In addition, this approach allows for a temporal lift simultaneously, which will elevate the lateral brow and avoid bunching of tissues in the temple. This way, the midface, lower lid, temples, and lateral brow are rejuvenated as a group, creating a more harmonious appearance. Initially, I combined this with a transoral approach to complete the dissection, but with more experience, I found this practice to be unnecessary, as I could get complete release of the midface from the temporal incision.
The preauricular approach can achieve midface elevation through a deep plane rhytidectomy dissection. In this approach, the SMAS layer is entered anterior to the frontal branch of the facial nerve and the dissection proceeds medially deep to the malar fat pad and superficial to the zygomaticus major muscle. After the zygomaticocutaneus ligaments are released, the malar fat pad can be elevated. The major advantage of the transtemporal approach over the preauricular approach is the vector of pull. The deep plane rhytidectomy has a more lateral vector, which is not optimal.
The transorbital approach also involves subperiosteal elevation of the midface soft tissue and its fixation to the deep temporalis fascia posterior to the orbital rim at a point just above the lateral canthus. The undermined skin-muscle flap elevated with the subciliary approach is then redraped and its excess removed. Following fixation and conservative excision of the lower lid skin, there is the need to create lower lid support, and this could be achieved with cathoplasty or a canthopexy, which can create several issues. Advocates for this technique claim that has the advantage of its dissection to avoid risk to branches of the facial nerve and create a vertical vector of pull. I don’t think the frontal branch is under high risk with the transtemporal approach, since in over 1000 cases I only had one case of permanent paresis that occurred during a complex revision procedure. Moreover, this technique carries a higher risk of lower lid malposition and creates bunching of soft tissue and skin in the lateral orbital rim, sometimes creating an unnatural appearance. The transtemporal approach, on the other hand, will increase lower lid support and the concurrent temporal lift will avoid this lateral bunching.
Sykes and Magill
The incision(s), approach, and fixation used to lift the midface are integrally related (ie, the incision used will affect the dissection plane and the method of flap fixation). There are several possible ways to approach the midface, including :
- 1.
Lateral temporal incision and approach
- 2.
Transblepharoplasty approach with a transconjunctival or transcutaneous incision
- 3.
Preauricular incision with a subcutaneous approach transitioning to a sub-SMAS plane
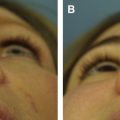
The advantages of a lateral temporal approach are the lateral vector of lift and the well-camouflaged incision. The transblepharoplasty approach provides good access to the midface, and a vertical vector of lift ( Fig. 3 ). The level of the inferior orbital rim is the superior limit of the lifting vector with the transblepharoplasty approach.
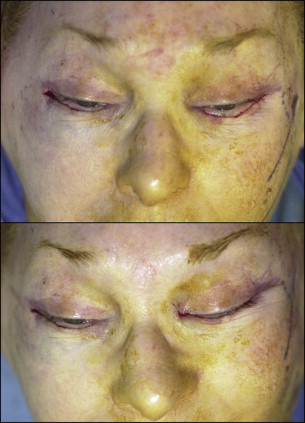
I prefer the preauricular incision with a subcutaneous preauricular dissection plane transitioning to a sub-SMAS plane at a line which joins the mandibular angle with the lateral canthus ( Fig. 4 ). The reason for not initially dissecting in the sub-SMAS plane is that the superficial and deep fascia are fused in the immediate preauricular region. The midface flap is then fixated to the deep temporal fascia.

What is the best incision/approach (preauricular, transtemporal, transoral)? Why?
Keller and seth
Generally, I prefer a temporal approach posterior to the hairline for lifting the midface. If the temporal incision is placed superior enough (close to the temporal line), an almost vertical direction of pull can be maintained. I will, on occasion, use an extended subciliary eyelid incision, in the face of severe temporal fascia scarring from previous procedures, though I can usually avoid this incision. An extended subciliary incision can produce an eyelid scar that needs to be covered with makeup, and can be associated with eyelid retraction and scleral show.
For positioning of an endotine in the proper position or for placing a malar implant, the intraoral incision is valuable. This incision gives the best access to the lower malar areas and the massateric tendon.
I will often use a transconjunctival incision to retroposition fat over the orbital rim, if orbital fat protrusion is a problem. Often, the orbital fat has protruded through a weakened septum, the globe has recessed, the SOOF fat has fallen, the orbicularis muscle has descended, and the malar fat pad has descended. Overall, this combination of aging effects produces the appearance of a “pot belly over fallen jeans.” This set of anatomic problems can occur even in the younger individual. While all ethnic groups exhibit this “pot belly over fallen jeans” phenomena, many people of Middle Eastern and Asian descent manifest it at a relatively young age.
Quatela and Antunes
Over the course of the years, I have used transoral, transorbital, and transtemporal approaches to achieve midface elevation. In my opinion, the best incision/approach is the transtemporal.
The transtemporal approach, as the name illustrates, achieves midface elevation through a small temporal incision. The dissection starts separating the deep temporal fascia from the deep layer of the superficial fascia and from there to the subperiosteal plane. The forehead and the zygomatic arch are elevated subperiosteally, and this way, as previously mentioned, the frontal branch is protected. The dissection proceeds inferiorly, elevating the soft tissues of the midface from the maxilla. This approach has several advantages over the preauricular and transorbital approaches due to its vector of pull, increased lower lid support, and avoidance of lower lid malposition. In addition, this approach allows for a temporal lift simultaneously, which will elevate the lateral brow and avoid bunching of tissues in the temple. This way, the midface, lower lid, temples, and lateral brow are rejuvenated as a group, creating a more harmonious appearance. Initially, I combined this with a transoral approach to complete the dissection, but with more experience, I found this practice to be unnecessary, as I could get complete release of the midface from the temporal incision.
The preauricular approach can achieve midface elevation through a deep plane rhytidectomy dissection. In this approach, the SMAS layer is entered anterior to the frontal branch of the facial nerve and the dissection proceeds medially deep to the malar fat pad and superficial to the zygomaticus major muscle. After the zygomaticocutaneus ligaments are released, the malar fat pad can be elevated. The major advantage of the transtemporal approach over the preauricular approach is the vector of pull. The deep plane rhytidectomy has a more lateral vector, which is not optimal.
The transorbital approach also involves subperiosteal elevation of the midface soft tissue and its fixation to the deep temporalis fascia posterior to the orbital rim at a point just above the lateral canthus. The undermined skin-muscle flap elevated with the subciliary approach is then redraped and its excess removed. Following fixation and conservative excision of the lower lid skin, there is the need to create lower lid support, and this could be achieved with cathoplasty or a canthopexy, which can create several issues. Advocates for this technique claim that has the advantage of its dissection to avoid risk to branches of the facial nerve and create a vertical vector of pull. I don’t think the frontal branch is under high risk with the transtemporal approach, since in over 1000 cases I only had one case of permanent paresis that occurred during a complex revision procedure. Moreover, this technique carries a higher risk of lower lid malposition and creates bunching of soft tissue and skin in the lateral orbital rim, sometimes creating an unnatural appearance. The transtemporal approach, on the other hand, will increase lower lid support and the concurrent temporal lift will avoid this lateral bunching.
Sykes and Magill
The incision(s), approach, and fixation used to lift the midface are integrally related (ie, the incision used will affect the dissection plane and the method of flap fixation). There are several possible ways to approach the midface, including :
- 1.
Lateral temporal incision and approach
- 2.
Transblepharoplasty approach with a transconjunctival or transcutaneous incision
- 3.
Preauricular incision with a subcutaneous approach transitioning to a sub-SMAS plane
The advantages of a lateral temporal approach are the lateral vector of lift and the well-camouflaged incision. The transblepharoplasty approach provides good access to the midface, and a vertical vector of lift ( Fig. 3 ). The level of the inferior orbital rim is the superior limit of the lifting vector with the transblepharoplasty approach.