Microvascular Free Transfer of A First Web Space Skin Flap of The Foot to Reconstruct The Upper and Lower Eyelids
L. A. CHAIT
The reconstruction of both upper and lower eyelids when their total loss accompanies orbital exenteration is difficult (1, 2). This deformity may result from tumor excision or trauma. For this reason, the use of a prosthesis that is either applied directly over the cavity or attached to spectacles is often advised. However, patients sometimes request reconstruction (Fig. 33.1).
INDICATIONS
The neurovascular free flap from the first web space of the foot has been invaluable in reconstructing both upper and lower eyelids in these instances (3, 4). The texture of the dorsal skin of the toes and the color match are found to be acceptable. The web itself forms a natural lateral canthus, and the thicker plantar skin gives enough support to maintain a light prosthesis. Crude sensation returns to the outer part of the flap. At first, this is referred to the temporal region, but later it tends to reorient to the eyelid itself. Both skin cover and lining for each of the upper and lower lids are provided in a single operation, and much of the scarring that results from local flap reconstruction can be avoided.
ANATOMY
See Chapter 335.
FLAP DESIGN AND DIMENSIONS
The flap includes the skin of the first web space of the foot, with extensions running onto adjacent toes as far as their tips. Enough skin must be removed from each toe to allow it to be folded on itself to provide both lid cover and lining. A small area of dorsal foot skin proximal to the web is included (Fig. 33.2). The flap must be taken from the foot on
the ipsilateral side, because the web has to provide the lateral canthus and the dorsal skin must be external.
the ipsilateral side, because the web has to provide the lateral canthus and the dorsal skin must be external.
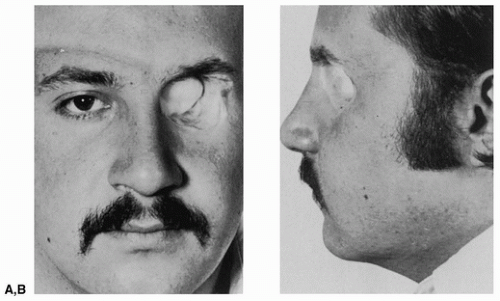 FIGURE 33.1 A,B: Patient 10 years after orbital exenteration for rhabdomyosarcoma. Socket was lined with a split-thickness skin graft.
Related posts: Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid Cheek Rotation Skin (Mustardé) Flap to The Lower Eyelid
 Wraparound Cartilage Flap for Correction of Cleft-Lip Nasal Deformity Wraparound Cartilage Flap for Correction of Cleft-Lip Nasal Deformity
 Oral Mucosal Flaps for Septal Reconstruction Oral Mucosal Flaps for Septal Reconstruction
 Postauricular and Retroauricular Scalping Flap (The Paras Flap) Postauricular and Retroauricular Scalping Flap (The Paras Flap)
 Platysma Musculocutaneous Flap to The Lower Lip Platysma Musculocutaneous Flap to The Lower Lip
 Microvascular Free Transfer of Serratus Anterior and Rib Composite Flap Microvascular Free Transfer of Serratus Anterior and Rib Composite Flap
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|