The mentolabial (or labiomental) fold is also known as the mentolabial sulcus. It is a region that is evident in frontal and profile view, forming the transition from the lower lip to the soft tissue chin. In frontal view the visible indentation responsible for the separation of the lower lip from the chin is known as the mentolabial groove or crease. The morphology of the mentolabial region is one of the most important aesthetic parameters of the lower face (Figure 18.1).
Mentolabial fold (sulcus) depth
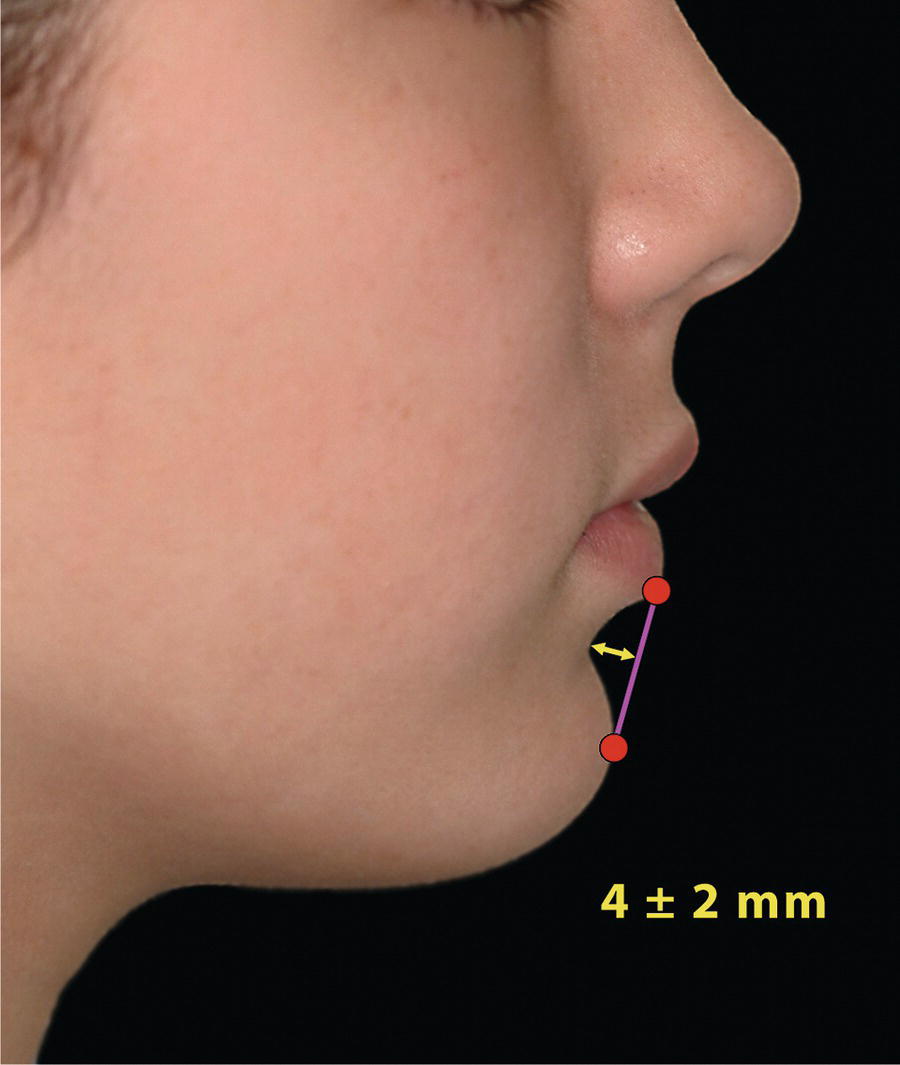
The depth of the mentolabial fold may be measured from the deepest point of the fold (sublabiale or soft tissue B‐point) with a horizontal line that is perpendicular to a vertical line from labrale inferius (vermilion border of the lower lip) to soft tissue pogonion (Figure 18.2).
The mentolabial fold depth may be slightly greater in men (6 mm) than women (4 mm) due to the greater chin prominence.
Figure 18.1 The morphology of the mentolabial region is an important aesthetic parameter of the lower face. (Detail, Study of the Head of a Woman, Leonardo da Vinci, c.1490, Musée du Louvre, Paris.)
Mentolabial angle
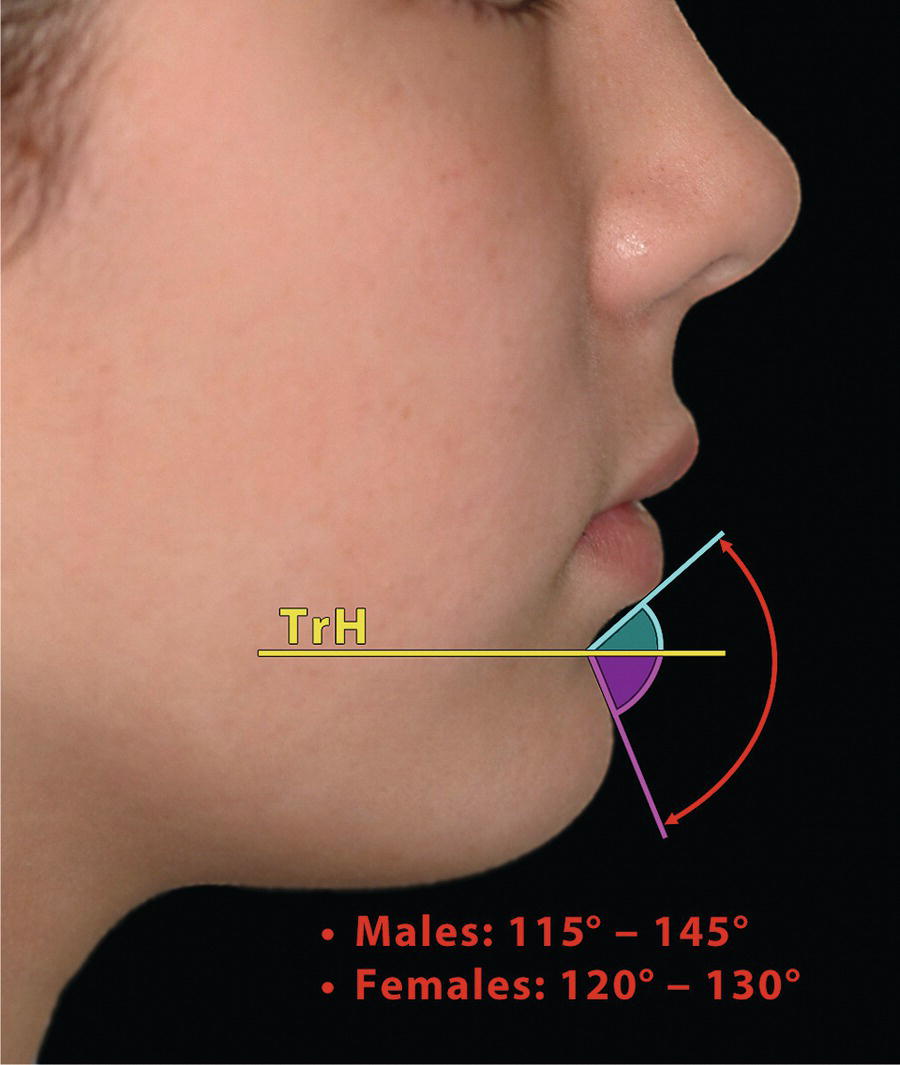
The mentolabial angle is the angle formed between the lower lip and soft tissue chin. The angle should be approximately 130°, but there is considerable individual variation (Figure 18.3):3
Males: 115°–145°
Females: 120°–130°
Like most facial profile angles formed between two neighbouring structures, the mentolabial angle may be divided into its two component angles by a true horizontal line drawn through sublabiale:
Figure 18.3 Mentolabial angle and its component parts. TrH, true horizontal plane.
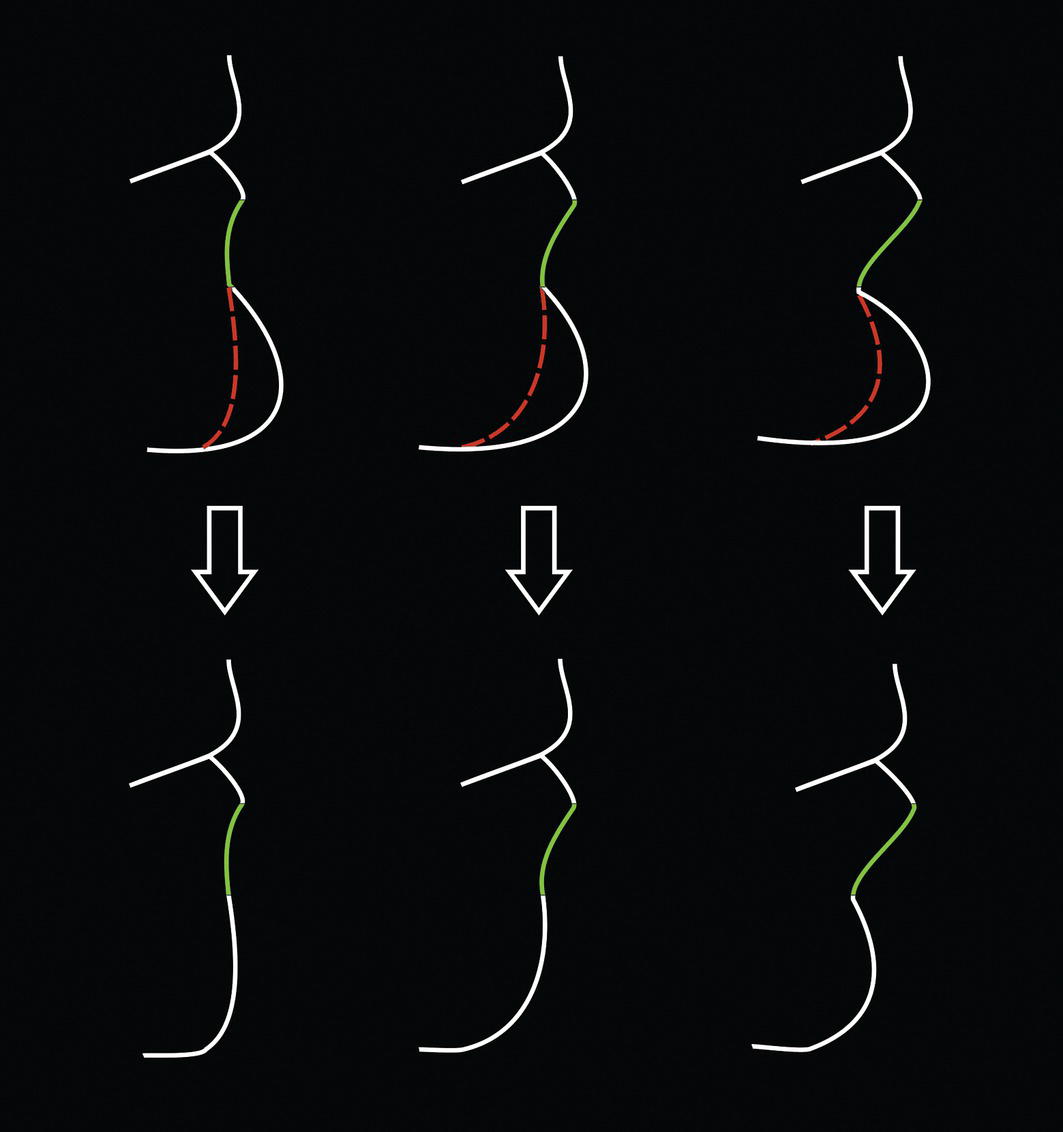
Upper component: This is the inclination of the lower lip in relation to the true horizontal line through sublabiale. It may be referred to as the lower lip‐to‐mentolabial crease inclination, or lip‐to‐crease incline.4 Normative values for this angle have been provided:3
Males: 47°–50° ± 18°
Females: 50° ± 14°
Figure 18.4 Variations in the inclination of the lower lip and corresponding results following horizontal reduction genioplasty.
(Redrawn from Zide and Boutros4/with permission of Wolters Kluwer Health.)
Lower component: This is the inclination of the soft tissue chin to the true horizontal line through sublabiale.
The mentolabial angle depends on one or a combination of the following factors:
Soft tissue factors:
Morphology of the lower lip: e.g. a flaccid, protrusive lower lip may reduce the mentolabial angle, whereas a thin, strap‐like lower lip will tend to increase the angle.
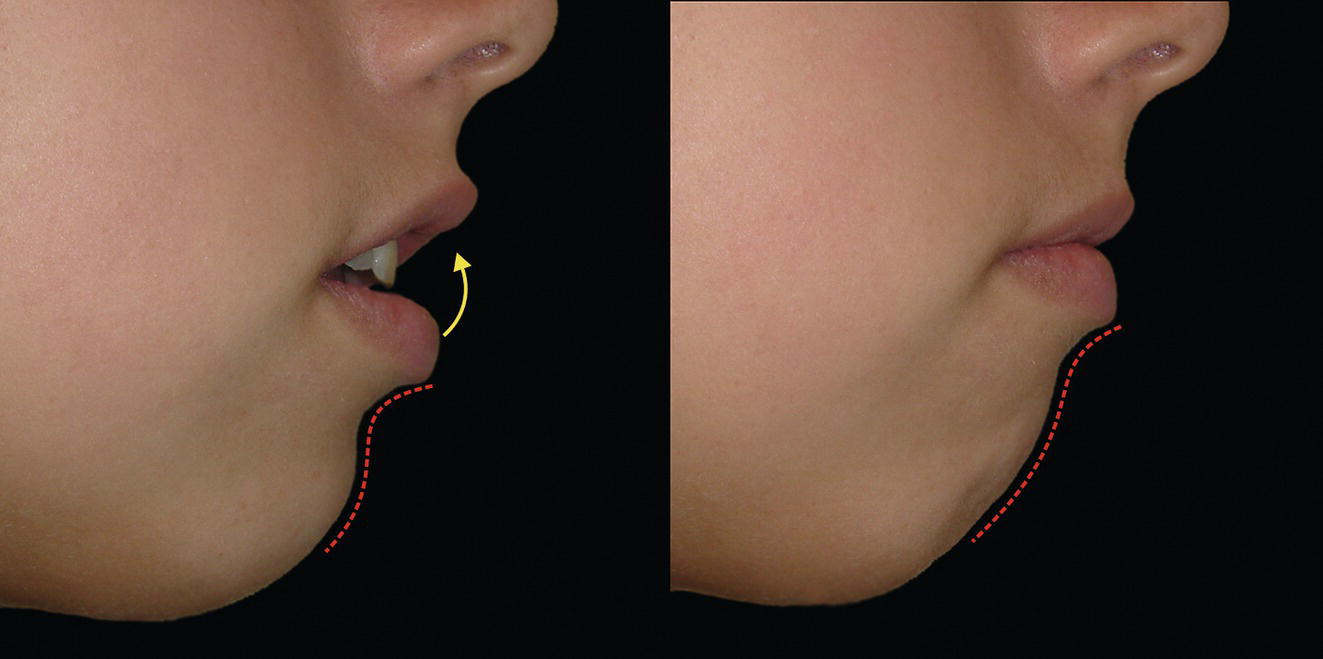
Figure 18.5 Patients with incompetent lip posture often elevate the lower lip in order to maintain a lip seal; this elevation, due to contraction of the mentalis muscle, tends to flatten the mentolabial fold.
Figure 18.6 Increased horizontal chin projection leads to a decrease in the mentolabial angle.
Lower lip posture: Patients with an incomplete lip seal (lip incompetence) have a tendency to elevate the lower lip in order to maintain a lip seal; this elevation, due to contraction of the mentalis muscle, tends to flatten the mentolabial fold (Figure 18.5).
Horizontal chin projection (due to increased thickness of soft tissue chin pad): Increased horizontal chin projection leads to a decrease in the mentolabial angle and vice versa (Figure 18.6).
Skeletal factors:
Horizontal chin projection (skeletal horizontal macrogenia): Increased horizontal chin projection leads to a decrease in the mentolabial angle and vice versa.
Lower anterior face height (LAFH): A reduction in LAFH may reduce the mentolabial angle, deepening the mentolabial fold. Conversely, an increase in LAFH may increase the mentolabial angle and reduce or even completely remove the mentolabial fold (Figure 18.7). The impact of such changes on the aesthetic contour of this area must be accounted for in treatment planning.
Dentoalveolar factors:
Inclination of the mandibular incisors: Proclined mandibular incisors will tend to protrude the lower lip; retroclination of the mandibular incisors may permit some retrusion of the lower lip, but this will depend to a great extent on the thickness and tonicity of the lower lip and the ability to achieve a competent lip posture.
Protrusion or retrusion of the mandibular dentoalveolus: The effect is as described above.
Anatomy of alveolar B‐point: i.e. if skeletal B‐point is set back, the mentolabial fold will tend to be deep and the angle reduced; if set forward in position, the mentolabial angle will tend to be increased.
Eversion of the lower lip by proclined maxillary incisors: In Class II patients with proclined maxillary incisors and reduced lower anterior face height, the maxillary incisors may impinge on the lower lip causing its eversion (Figure 18.8).
Only gold members can continue reading. Log In or Register to continue