Introduction
Scar formation is an essential part of wound healing. Following injury to the skin, wound healing occurs in four stages: hemostasis, inflammation, proliferation, and tissue remodeling. It is during the tissue remodeling stage that the mature scar is produced and type III collagen (granulation tissue) is replaced with type I collagen. In pathologic scarring, there is excessive fibroblast and myofibroblast proliferation resulting in collagen deposition, which may lead to either a keloid or hypertrophic scar. Both are characterized by a state of chronic inflammation. Keloids and hypertrophic scars have been shown to have a significant impact on quality of life and a high disease burden. In addition to being aesthetically bothersome, scars may also lead to pain, erythema, pruritus, contractures, and functional impairment.
Medical scar treatment encompasses a wide range of modalities ( Table 2.1 ). In 2022, the global scar treatment market was valued at $23.5 billion and is predicted to increase at a 9.9% compound annual growth rate from 2023 to 2030. A systematic review evaluating 25 randomized controlled trials (RCTs) conducted through 2019 concluded that there was only a mean absolute improvement of 44.4% across all scar treatments, thus highlighting the need for better therapies. This chapter will focus on medical treatments including physical modalities, topical treatments, and intralesional therapies. These are often the most accessible therapies in the clinic setting and are considered first line for scar therapy.
| Manual Therapy | Topical Therapy | Intralesional Therapy |
|---|---|---|
|
|
|
Manual Therapy
Pressure and Compression Therapy
Pressure and compression therapy ( Figs. 2.1 and 2.2 ) are commonly employed scar therapies proposed to work via hypoxia and apoptosis of scar tissue by modulating interleukin-1β and transforming necrosis factor-alpha. Despite their consistent presence in many scar treatment algorithms and recommendations, objective data regarding their efficacy are lacking. One recent meta-analysis evaluated scars caused by multiple different etiologies, and the analysis found no improvement across multiple scar scales with use of compression therapy alone. A more recent RCT examined the effects of silicone, compression, and silicone with pressure garment therapy in pediatric burn patients. No significant difference was found among the three groups. Despite a lack of objective data, pressure and compression therapy remain a low-risk, low-cost component of many treatment algorithms, especially for burn victims. The scenario with the best evidence for pressure therapy is following keloid excision, particularly of the ears. Pressure therapy has been shown to decrease rates of keloid recurrence following surgical excision, and patients can purchase individualized clips to wear daily.

Massage Therapy
Manual massage therapy ( Box 2.1 ) is another popular technique recommended in scar treatment and prevention, particularly for burn victims. Massage is thought to help with realigning the extracellular matrix proteins leading to improved tissue pliability. However, the data are conflicting. Several studies cite improvement in scar elasticity, erythema, melanin, thickness, pain, and itch, whereas others counter this and report minimal to no improvement. One recent well-designed RCT on adult burn scars showed that these parameters improved initially, but there was no long-term benefit with 5 minutes of massage per day. Another study reported that patients who demonstrated improvement with scar massage had more hypertrophic and erythematous scars and performed scar massage for 30 minutes per day. Scar massage may also reduce patient anxiety, distress, itch, and pain surrounding a noticeable scar. Interestingly, timing seems to be an important factor in treatment outcomes. Animal models have shown that massage done in earlier phases of wound healing causes more hypertrophic scars. Data suggest the earliest patients should consider massage therapy is around the end of the proliferative phase (∼14 days postoperatively). Nevertheless, when done correctly, the risks of scar massage appear to be minimal. Objective data for timing and frequency of massage are lacking.
- 1.
Clean the hands.
- 2.
Apply an emollient such as petrolatum to the fingers.
- 3.
Using the pads of the fingers, massage for 15 minutes twice per day in all directions (up and down, side to side). Use as much pressure as possible without causing pain. Scars generally only reach about 70% to 80% of the skin’s normal strength so the skin can easily be injured.
- 4.
If there is pain, bleeding, or wound dehiscence, stop.
- 5.
Continue for 3–6 months or until the scar is pink and flat.
Topical therapy
Numerous topical therapies have been tried for keloids and hypertrophic scars including sunscreen, silicone gel/sheets, vitamin E, onion extract, and immunomodulators. All therapies will be touched upon briefly except for vitamin E. Clinical studies evaluating vitamin E have shown underwhelming results and a high prevalence of allergic contact dermatitis. As a result, topical vitamin E is not recommended in any scenario.
Sunscreen
Sunscreen is recommended for all patients. An RCT in 2006 documented the negative effects of ultraviolet (UV) light exposure on healing wounds. In this trial, 14 patients underwent punch biopsy on the gluteal region and were then randomized to heal by either primary or secondary intent and then randomized further to UV-exposed or non–UV-exposed groups. Patients in the UV group were exposed to an amount of UV light analogous to sitting at a Denmark beach in the summer for 30 minutes. Researchers saw worse scar discoloration, more inflammation under histology, and larger-sized scars in the group exposed to UV radiation. As such, all patients should wear sunscreen to protect against the negative effects of UV light. The authors recommend at least SPF 30, preferably a mineral sunscreen containing zinc oxide and/or titanium dioxide.
Silicone Gel and Silicone Gel Sheets
Silicone gel and sheets ( Box 2.2 ) are the topical conservative modality assessed most frequently in the literature for scar prevention and treatment. Silicone products are composed of synthetic polymers containing a silicon-oxygen backbone and organic groups. These materials come in a fluid, gel, or rubber form and are safe and well tolerated. The mechanism of action is unclear. However, the leading theory is that silicone products occlude and hydrate the wound, minimizing capillary activity, hyperemia, and ultimately collagen deposition. Potential adverse events are mild and more common in hot, humid environments. These may include irritation, pruritus, skin rash, maceration, and dryness.
- 1.
Silicone gel and sheets are easily available by prescription or online.
- 2.
Apply directly over the scar. They may be cut with scissors to the shape of the scar both for cost-effectiveness and cosmesis. The authors recommend opaque sheets for the added benefit of sun protection.
- 3.
Wear the sheets for 12–24 hours per day. Gel sheets can be washed after a 24-hour application.
- 4.
Silicone gel is often applied two to three times per day. The gel may be better for concave and convex surfaces.
There is some data in support of silicone sheets in the literature. According to a Cochrane review, silicone sheets may reduce the risk of hypertrophic scars and keloids in persons who are susceptible (risk ratio 0.46, 95% confidence interval [CI] 0.21–0.98). Silicone dressings may also improve color (summary risk ratio 3.49, 95% CI 1.97–6.15) and softness (summary risk ratio 3.03, 95% CI 1.02–8.99). The reviewers highlight that the currently available data are overall low quality and susceptible to bias. Therefore, these conclusions should be interpreted with caution and the cost-effectiveness of this treatment should be taken into account. Studies show similar efficacy for silicone gel and sheets. Of note, the gel must be allowed to dry and has to be applied multiple times per day. Some advocate the use of gel in cosmetically sensitive areas. For patients who opt to use silicone products, earlier use and longer duration seem to lead to better results.
Onion Extract ( Allium Cepa )
There are many clinical studies evaluating the efficacy and tolerability of onion extract ( Box 2.3 ). Allium cepa is the active ingredient and is postulated to suppress scar formation via antiproliferative and antiinflammatory properties. Efficacy rates in scar prevention, reduction, and symptomatic improvement are highly variable. In a randomized, double-blind, split-scar study, Chung et al. compared petrolatum emollient to onion extract gel application following surgery and failed to find statistical differences between both groups. Similar findings were seen by Jackson and Shelton in ameliorating postsurgical scar symptoms and erythema. More recently, a group in Switzerland performed an RCT evaluating onion extract hyaluronic acid 5% gel versus silicone gel. They found improvements in itching and redness at 4 and 8 weeks with the onion extract gel compared to the silicone gel group.
- 1.
Purchase an over-the-counter product such as Mederma Advanced Scar Gel or Contractubex gel.
- 2.
Apply twice per day for up to 3 months.
The more favorable data in support of onion extract are found when used in combination with other treatments. Hosnuter et al. evaluated the therapeutic efficacy of onion extract gel for hypertrophic and keloid scars compared to and in combination with silicone gel sheets. Onion extract again provided greater improvements in scar color, whereas silicone gel sheets led to greater improvements in scar height. Combined silicone gel sheets and onion extract therapy produced the most favorable results. Similarly, in one small, single-blind RCT, clinicians determined that intralesional 40 mg/mL triamcinolone (TAC) injections (administered every 4 weeks four times total) in combination with an onion extract gel (Contractubex) applied three times per day for 3 months showed greater improvements in pain, itching, and scar elevation, but not in erythema or induration compared to intralesional 40 mg/mL TAC alone administered at the same frequency . Ultimately, while there may be a role of onion extract with heparin and allantoin in scar prevention, the available data are weak.
Topical immunomodulators
Imiquimod
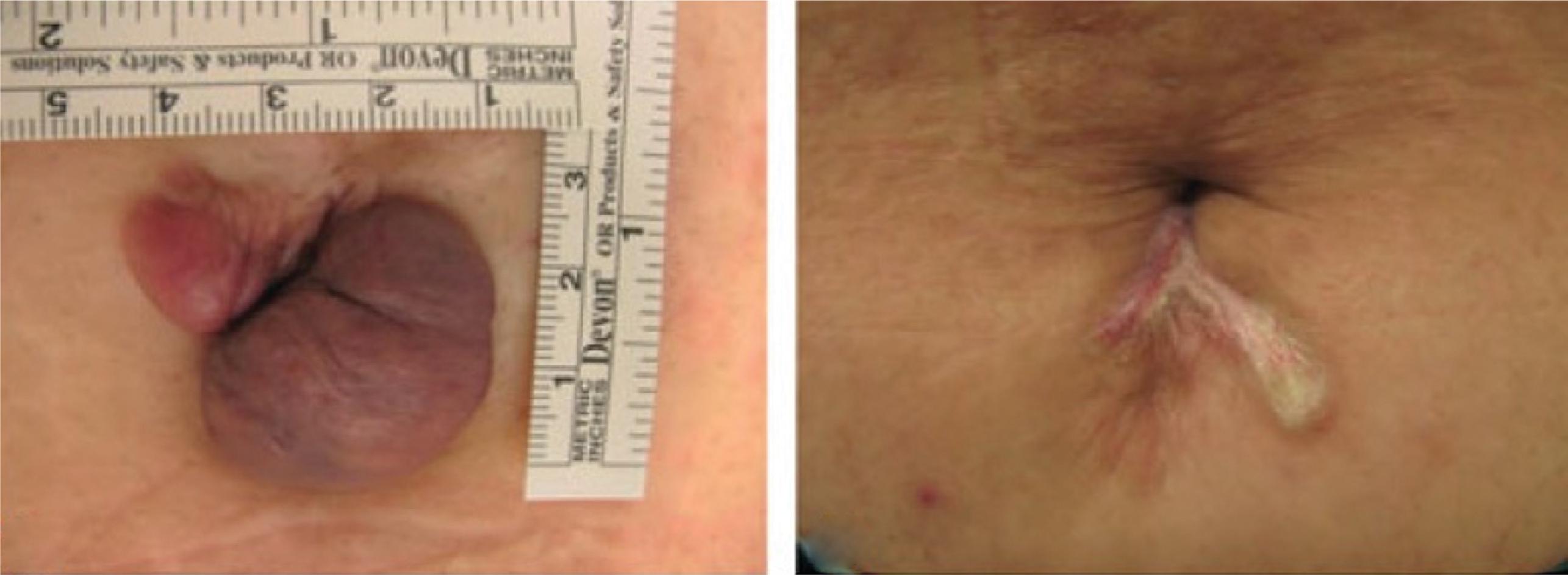
Imiquimod is a toll-like receptor 7 activator that may be helpful following keloid excision ( Fig. 2.3 , Box 2.4 ). In an uncontrolled pilot study, eight keloids located on the ear were treated with excision and adjuvant topical 5% imiquimod daily for 6 weeks. At 1 year postoperatively, no lesions recurred, and the patients denied any pain or itching at the prior keloid sites. Other small studies have shown similar efficacy in treating stubborn ear keloids, but further research and larger trials are warranted at the present time.

- 1.
Imiquimod 5% cream must be prescribed.
- 2.
Beginning the night of surgery, clean the healing wound and apply a thin layer of imiquimod 5% cream. Place a dressing on top of the healing wound.
- 3.
In the morning, remove the dressing, clean the wound, and apply petrolatum during the day.
- 4.
Continue nightly a for up to 6 to 8 weeks as tolerated.
- 5.
Watch for hyperpigmentation and skin abrasions as well as systemic side effects of imiquimod including fever and lymphadenopathy.
Mitomycin C
Mitomycin C ( Fig. 2.4 , Box 2.5 ) is an antitumor antibiotic with antifibroblastic properties. Similar to imiquimod, most of the available data for use describes its applications in treating keloids. Mitomycin C has been investigated both as a topical and an intralesional agent. The largest study evaluated topical therapy applied to 26 ear pinna keloids following excision. Patients were treated with topical mitomycin C (1 mg/mL) at the time of surgery for 3 minutes and again at 3 weeks, with no recurrences seen at 2-year follow-up. Interestingly, in another study, patients who underwent intralesional mitomycin C developed ulceration and keloid progression. Potential side effects of topical mitomycin C include prolonged wound healing, hyperpigmentation, posttreatment pain, and skin atrophy.
- 1.
Perform shave excision with secondary intent wound healing.
- 2.
Prepare 1 mg/mL mitomycin C solution by adding 2 mL sterile water to 2 mg mitomycin C powder. a
- 3.
Apply mitomycin C–soaked gauze to the wound.
- 4.
Let sit on the open wound for 3–5 minutes.
- 5.
Remove the gauze, pat dry, and apply a clean dressing.
- 6.
Mitomycin C application can be repeated at 3 weeks if indicated.
Cryotherapy
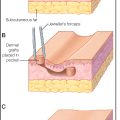
Cryotherapy has shown promise in the treatment of keloids and hypertrophic scars by causing direct cell injury through cellular dehydration with the formation of ice crystals, which subsequently cause organelle and cell membrane damage and resultant keloid necrosis and collagen reorientation. It has been shown that 51% to 74% of patients achieve keloid flattening after two or more cryotherapy sessions. However, its utility is limited by its side effect profile, including pain, prolonged healing time, skin dyspigmentation, and skin atrophy. Two modified algorithms attempt to address these limitations: (1) short-duration contact cryotherapy followed by intralesional corticosteroids and (2) intralesional cryotherapy ( Box 2.6 ). With the first option, contact cryotherapy acts synergistically with intralesional corticosteroids by creating dermal edema and facilitating drug delivery, increasing efficacy up to 86%. Intralesional cryotherapy ( Fig. 2.5 ) is also effective and creates less pigment alteration compared to traditional contact cryotherapy.
For both options, counsel patients that cryotherapy can cause blistering or crusting, which are expected side effects and not worrisome. These side effects are more common with contact cryotherapy.
Option 1: Contact cryotherapy and intralesional corticosteroids
Cryotherapy can be applied with a cotton swab or a handheld spray unit. One study administered cryotherapy for two freeze-thaw cycles of up to 30 seconds each immediately prior to injection of steroid (see Box 2.7 for injection technique). Shorter duration freeze cycles may also be efficacious.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


