Introduction
Increasing knowledge of the blood supply to the distal femur has resulted in the development of a variety of composite flaps designed to include bone from the medial femoral condyle. Flaps from this area can be designed to include not only bone but also articular cartilage, skin, muscle, and tendon. The original description of a periosteal flap from this region was described by Masquelet in 1988 and was based on the descending geniculate artery. This flap was then modified by Doi to include the periosteum and femoral cortex for the management of scaphoid non-unions. Recent publications have shown the medial geniculate arterial system also supplies the surrounding skin, articular cartilage, muscle, and tendon allowing for the creation of composite vascularized bone flaps. This variation in tissue types, in addition to a relatively small donor site, has allowed this flap to gain a newfound popularity for the management of composite bony defects within the extremities as well as the head and neck as its donor site may compare favorably with that of the fibula or iliac crest bone flaps.
Flap Anatomy ( Figs 55.1 , 55.2 , see Fig 13.1 , Fig 13.2 , Fig 13.4 , Fig 13.19 )
The flaps of the medial femoral condyle (MFC) are based on the geniculate arterial system, which is a branch of the femoral artery and is located medially in the thigh and knee.
Arterial Anatomy of the Flap ( Figs 55.1 and 55.2 , see Figs 13.2 and 13.4 )
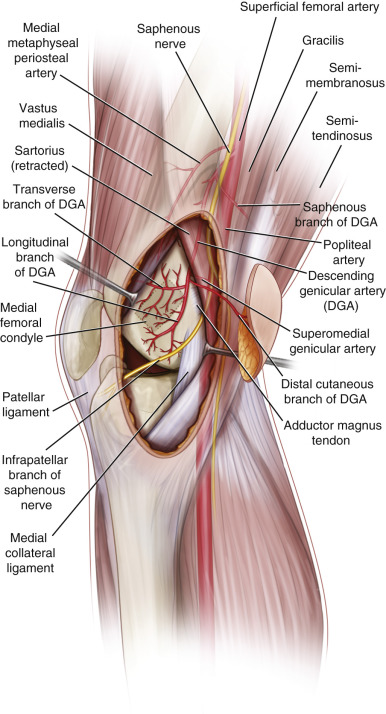
The anatomy of the MFC flap has been studied extensively and most recently by Yamamoto and Iorio and colleagues. The bone flap is located over the medial femoral condyle and is bound by three borders, the posterior border of the femur, anteriorly by the medial patellar facet, and distally by the medial collateral ligament. The flap is supplied by two sources: the descending genicular artery (DGA) and the superomedial genicular artery (SGA). The DGA originates from the femoral artery just distal to the adductor hiatus. It lies deep or lateral to the adductor magnus tendon along the posterior aspect of the medial intermuscular septum. The DGA typically has three branches, including an articular branch, a muscular branch, and a saphenous branch. The articular branch feeds the periosteum and the articular cartilage on the superior femoral condyle. The muscular branch supplies the vastus medialis muscle and the saphenous branch supplies the subcutaneous tissue and overlying skin.
Yamamoto and colleagues studied the arterial anatomy to the medal femoral condyle in 19 cadavers. They discovered the DGA was present in 89% of the specimens with the artery originating on average 13.7 cm from the articular surface of the knee. At its origin the vessel had an average internal diameter of 1.5 mm (range 1–2 mm). An osteoarticular branch was present in 89% of specimens branching from the DGA approximately 11.3 cm (range 5.5–15 cm) from the knee joint and this branch had an average internal diameter of 1.1 mm (range 0.63–1.5 mm); 79% of specimens had an identifiable saphenous branch, which travels with the saphenous nerve and perfuses the overlying skin.
The SGA originates from the proximal portion of the popliteal artery. In Yamamoto’s anatomic study, this vessel was present in 100% of the specimens with the origin of the vessel just 5.2 cm from the articular surface. The vessel has an average internal diameter of 0.78 mm at its origin and ranged in diameter at 0.38–1.4 mm. The vessel crosses from behind the adductor magnus tendon to anastomose with the osteoarticular branch of the DGA contributing to the perforating vessels over the condyle. The superior medial genicular artery was the dominant vessel supplying the medial femoral condyle in two of the specimens in Yamamoto’s study ( Fig. 55.2 ).
Additional pertinent anatomic points about the flap include:
- •
The preferred vascular supply to the flap is the DGA, as it has a longer pedicle length (between 5 and 10 cm), and larger internal diameter than the SGA, facilitating microvascular anastomosis.
- •
The DGA divides into three arteries: the muscular branch, the articular branch, and the saphenous branch.
- •
The articular branch divides into the upper transverse artery (UTA) and the central longitudinal artery (CLA):
- •
The UTA gives off four branches: ascending, posterior descending, middle descending, and anterior descending branches
- •
The CLA divides into the posterior (arcuate) and anterior branch.
- •
- •
The middle branch of the UTA and the anterior branch of the CLA anastomose to form the main anastomotic arch of the medial femoral condyle.
Dominant:
descending geniculate artery (DGA)
Distance from the medial knee joint line: 15.4 cm (11.3–20.8 cm)
Diameter: 1.5 mm (1–2 mm)
Length: 1.2 cm (0.3–3 cm)
The descending geniculate artery is absent or diminutive in 10–15%.
Secondary:
superior medial geniculate artery (SMGA)
Distance from the medial knee joint line: 7.5 cm (4.7–9 cm)
Diameter: 0.75 mm (0.29–1.3 mm)
Muscular Branch of the DGA
Distance from the medial knee joint line: 12 cm (8–18 cm)
Diameter: 1.4 mm (0.5–3 mm)
Length: 6.3 cm (5–7 cm)
Articular Branch of the DGA
Distance from the medial knee joint line: 12.5 cm (10–17.5 cm)
Diameter: 1.2 mm (0.5–1.8 mm)
Length: 11.4 cm (6.5–14 cm)
Saphenous Branch of the DGA
Distance from the medial knee joint line: 13 cm (9–17.5 cm)
Diameter: 1.3 mm (0.4–2 mm)
Length: 13.7 cm (10.5–16 cm)
Arterial Supply of Periosteum
Upper Transverse Artery (UTA)
Distance from the medial knee joint line: 7.2 cm (5.4–8.9 cm)
Diameter: 0.55 mm (0.38–0.70 mm)
Branches of the UTA
Middle Descending Branch
Distance from the UTA takeoff of the descending genicular artery: 2.7 cm (1.4–7 cm)
Diameter: 0.28 mm (0.21–0.29 mm)
Anterior Descending Branch
Distance from the UTA takeoff of the descending genicular artery: 0.96 cm (0.3–1.6 cm)
Diameter: 0.33 mm (0.18–0.41 mm)
Central Longitudinal Artery (CLA)
Length from the UTA takeoff of the descending genicular artery: 3.4 cm (1.7–5.3 cm)
Diameter: 0.49 mm (0.31–0.67 mm)
Branches of the Cla
Anterior Branch
Distance from the CLA origin of the descending genicular artery: 1.98 cm (0.4–4.1 cm)
Posterior Branch
Distance from the CLA origin of the descending genicular artery: 2.59 cm (0.8–4.65 cm)
Angiosome of the Skin Paddle
Descending Geniculate Artery Distal Cutaneous Branch
Angiosome area: 70 cm 2
Saphenous Branch
Angiosome area: 361 cm 2
Venous Drainage of the Flap (see Fig. 13.19 )
The medial femoral condyle is drained by the corresponding venous comitantes that run with the descending and superomedial genicular arteries. Each of these arteries has two corresponding venous comitantes. The skin is drained by cutaneous perforating braches of the descending genicular vein as well as the saphenous vein. These arteries then drain into the superficial femoral vein.
Primary:
dual concomitant veins of the descending geniculate artery
Secondary:
dual concomitant veins of the superior medial geniculate artery
Length: 2–6 cm or longer
Diameter: 2–4 mm
Flap Innervation (see Figs 55.1 , 13.1 , 13.19 )
The skin of the medial knee is supplied by the saphenous nerve. This nerve provides sensation to the knee and upper medial lower leg as well as the medial aspect of the knee joint proper. The saphenous nerve travels with the descending geniculate artery in the adductor hiatus under the sartorius.
Medial Femoral Cutaneous Nerve
Distance from the medial knee joint line: 12.9 cm (9–15 cm)
Saphenous Nerve
Distance from the medial knee joint line: 7.8 cm (4–8 cm)
Sensory:
The cutaneous skin is supplied by branches of the saphenous nerve. There are limited reports of the use of neurovascular free flap based off the saphenous neurovascular pedicle.
Motor:
This flap can include portions of the vastus medialis; however, there are no reports of functional muscle transfer.
Flap Components
The flap is extremely versatile. Historically this flap was created to carry the periosteum from the femur but can now be used to carry corticocancellous bone, articular bone, portions of the vastus medialis, skin, saphenous nerve, and portions of the adductor tendon.
Advantages
- •
The MFCF has several positive attributes, the first being a relatively consistent arterial pedicle of large size (1.8–2.2 mm) and sufficient pedicle length (4 cm).
- •
Two teams may work simultaneously allowing for flap harvest and preparation of the recipient site.
- •
Can be used for articular surface reconstruction of the carpus.
Disadvantages
- •
Limited size (12 × 14 cm), which makes the flap inadequate for larger reconstructive problems.
- •
There is a possibility of injury to the knee with stiffness, instability, and early arthritis, though the true incidence has not been reported.
Preoperative Preparation
There are few requirements for preoperative imaging when using this flap. The anatomy (discussed above) is very reliable. Attention instead is given to the non-union site to verify the size of the defect, the bony dimensions required for reconstruction, and to rule out evidence of ongoing infection. In general, preoperative imaging is performed for the following circumstances:
- •
Preoperative assessment of non-unions and carpal collapse can be assessed with a CT scan of the hand and wrist. MRI with gadolinium contrast can help assess for signs of avascularity, most commonly encountered in Kienböck disease or proximal pole fracture of the scaphoid. In addition, preoperative CT scans of the non-union site allow for templating of the required graft dimensions.
- •
CT angiography or an MRA can be considered in patients with previous knee surgery, significant peripheral atherosclerotic disease, or previous knee trauma, to verify the patency of the geniculate arterial system.
- •
There has been one case of a chronic DGA thrombosis, which resulted in aborting the free flap. The authors recommended considering a CT angiogram or MRA to evaluate the DGA in high-risk patients as noted above. They also suggested evaluating the DGA pedicle at the time of harvest for signs of chronic thrombosis.
- •
Flap Design ( Fig. 55.3 )
Anatomic Landmarks
A point between the medial aspect of the patella and the prominence of the medial femoral condyle marks the distal aspect of the incision. A longitudinal line is marked proximally and over the adductor hiatus.
General Thoughts About Flap Design
Historically, vascularized bone grafts such as the fibula, rib, or iliac crest have been used when bony defects exceed 5 cm in length. Unfortunately, non-union sites <5 cm in length, particularly those that are in areas of preexisting infection, avascular necrosis, or radiation, may be unamenable to the use of non-vascularized bone grafts and may require vascularized bone grafts to obtain bony union. In such situations, the classic sources of vascularized bone grafts, such as the fibula or iliac crest, are excessive in size resulting in unnecessary donor site morbidity and prolonged rehabilitation. For these specific circumstances, we have opted to use the medial femoral condyle corticoperiosteal flap. The medial femoral condyle corticoperiosteal (MFC) flap can provide a versatile source of vascularized bone with limited donor site morbidity and requires minimal time for flap harvest.
Although a periosteal flap can be elevated alone (without the underlying bone), disrupting the strongly adherent Sharpey fibers between the periosteum and cortex risks injury to the cambium layer; injury to this layer decreases the osteogenic potential of the graft. As such, studies have recommended including a layer of cortex when harvesting the flap, thus minimizing this risk of injury to the cambium layer.
Special Considerations
- •
The SGA, while smaller in diameter than the DGA, is still a very reasonable option when longer pedicle length is not required, as in cases of Kienböck disease and some cases of scaphoid non-union. In addition, the SGA has a good diameter vessel match when performing end-to-end anastomosis to side branches of the radial artery.
- •
An average of 30 arterial perforators to the medial femoral condyle has been reported. The perforating vessels run perpendicular to the cortex over an average area of 19 cm 2 , extending to an average depth of 13 mm. The majority of perforators lie in the posterior medial quadrant of the condyle. Care should be taken to identify these perforators and include them within the bone flap
- •
If a skin paddle is to be taken with the flap, it is necessary to separate the saphenous nerve from the saphenous branch of the DGA. Injury to this nerve will result in paresthesia or dysesthesias over the anterior medial aspect of the parapatellar/pretibial region of the leg.
- •
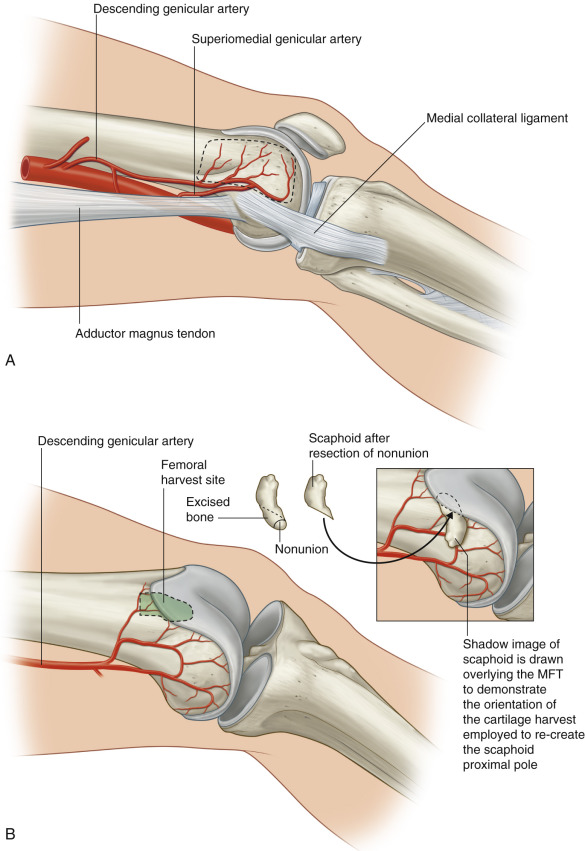
The convex articular surface of the medial femoral trochlea has a similar radius of curvature to carpus, specifically the proximal scaphoid and lunate.
Relative contraindications may include radiation to the region of flap harvest, or significant peripheral vascular disease involving the adductor canal or popliteal area, as these may compromise the arterial pedicle to the flap. Previous knee surgery, which has injured or ligated the geniculate arterial system, which feeds the MFC flap, will prevent the successful use of the flap.
Other patient-specific contraindications in cases of scaphoid non-union, Preiser disease, and Kienböck disease, would be the existence of wrist arthritis. In such cases, once wrist arthritis is established, bony revascularization or bony union will not alleviate the patient’s pain. In such cases, some form of intercarpal fusion is usually indicated.
Difference in Design, If Any, When Performing the Flap as Pedicled or Free
The design is similar in either case, although there are rare indications for pedicled flaps from this region.
Flap Dimensions
Skin Island Dimensions
Length: average 3 cm (range 2–8 cm)
Width: average 3 cm (range 2–8 cm), maximum to close primarily 2–4 cm
In most cases, a small skin island is taken for flap monitoring. This skin island is excised at a later date.
Bone Dimensions
Length: average 5 cm
Width: average 3 cm
Thickness: average 3 cm
The MFC flap should not be the first choice in cases where the bony defect is >3 × 5 cm. LaPierre et al. has described using MCF grafts with dimensions as large as 13 × 8 cm. These findings have been further validated by Iorio, who in a cadaveric study found that the geniculate system may be capable of perfusing flaps of up to 13 cm in length 8. Despite these findings, we would recommend using a graft with more structural integrity if the bony defect extends beyond 3 × 3 cm.
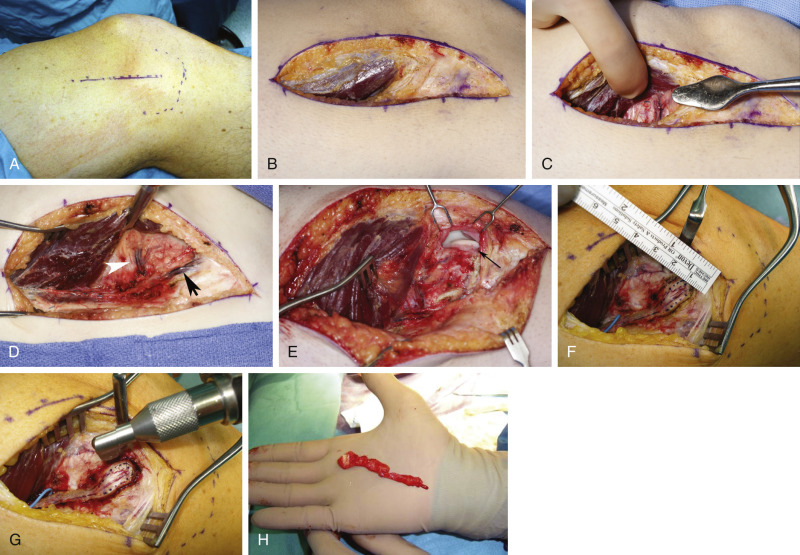
Flap Markings ( Fig. 55.3A , 55.7B )
Doppler ultrasonography is used to map the perforators in the region. A small skin island is designed over the Dopplered perforator.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


