Measuring meaningful outcomes in cleft lip and palate surgery is difficult. Many methods of measurement lack validity or reliability, are impractical to implement, or are not consistently used. Yet the power of measuring outcomes is so great, and the potential to improve patients’ lives so strong, that these hurdles are worth overcoming. This chapter reviews previous efforts at outcome measurement from cleft centers around the world. It also suggests a framework for adopting outcome measurement within your practice. Challenges of measurement are discussed, along with the role outcome reporting will take in accreditation and quality management.
Key points
- •
Outcome measurement is essential to document quality and to facilitate improvement.
- •
Cleft surgeons should choose outcome measures that are valid, reliable, practical to implement, and broadly adopted.
- •
New measures are under development, and existing measures will continue to evolve in all aspects of cleft care. Measures should focus on outcomes most relevant to patients and include input from providers and health care purchasers.
If you can not measure it, you can not improve it.
Why measure outcomes?
Once the sole purview of clinical and health-services research, outcome assessment has become a core component of clinical practice. Generally speaking, outcome measurement may be used for accountability, quality improvement, and health-system design (eg, resource allocation, purchasing decisions, and policy development) ( Box 1 ). Accountability refers to the demonstration that a particular surgeon’s or team’s results are within accepted standards. Quality improvement is a process of combining domain expertise with knowledge of systems, variation, and psychology to effect meaningful improvement. Originally developed in the manufacturing and service industries, quality improvement is now widely applied to health care delivery systems.
Accountability
Accreditation
Quality assurance
Public reporting
Quality improvement
Improve clinical care
Research
Board certification
Health-system design
Resource allocation
Value-based purchasing
Policy development
It is intuitive that regularly reviewing one’s outcomes is useful and instructive for improving patient care. For some time, the American Board of Medical Specialties’ Maintenance of Certification process has required demonstration of quality-improvement practices in an individual’s clinical practice. However, it is important to underscore that routine collection and reporting of clinical outcomes are increasingly emphasized in the public sphere. There is a growing movement to tie reimbursement to outcomes, and organizations such as the Leapfrog group and the Agency for Healthcare Research and Quality have advocated public reporting of these data. The American College of Surgeons’ National Surgical Quality Improvement Program was conceived as a volunteer program to help hospitals monitor specific clinical outcomes (particularly the so-called never events) that are already being tied to reimbursement. Recently, the Centers for Medicare and Medicaid Services announced its intention to require a proven level of performance to be eligible for payment. In the future, payers will be increasingly sensitive to objective data on outcomes when deciding where care should be directed and when negotiating fees.
Outcomes assessment and quality improvement requirements in cleft care
Specific to cleft care, the American Cleft Palate Association (ACPA) established minimum requirements for accreditation. These requirements include that “the Team has mechanisms to monitor its short-term and long-term treatment outcomes” by documenting “its treatment outcomes, including base-line performance and changes over time” and conducting “periodic retrospective or prospective studies to evaluate treatment outcomes.” Similar requirements exist in the United Kingdom. To date, the ACPA offers no specific recommendations regarding which outcomes should be assessed, nor how these data are to be collected, analyzed, and interpreted. Consequently, the onus is on each cleft team to conceive and develop its own system of outcomes assessment, monitoring, and quality assurance.
Outcomes assessment in the literature
Cleft lip and palate treatment has been the subject of innumerable studies in the surgical, medical, and allied health literature. Most of the evidence base is level IV and level V evidence—that is, most data derive from case series, experiential reports, and expert opinion. Few papers have been subjected to the rigors of contemporary clinical trial design or systematic review and metanalysis.
Some outcome data do exist. Perhaps the most complete early report was a 1984 study by Bardach and colleagues describing the long-term esthetic, dental, facial growth, and speech outcomes of 45 patients with unilateral cleft lip and palate. In 1987, the Third International Symposium on Early Treatment of Cleft Lip and Palate initiated a collaborative investigation, in which cephalograms and treatment records from 15 international centers were reviewed to evaluate the effects of individual treatment protocols on facial growth. Attendees from the symposium later developed novel measures for objective comparison of treatment outcomes, such as the Great Ormond Street, London, and Oslo (GOSLON) yardstick for assessing dental arch alignment and a validated instrument for rating nasolabial esthetic results.
In the late 1980s and early 1990s, Eurocleft was founded to study treatment outcomes from 6 European cleft centers. The Eurocleft study included Caucasian children with nonsyndromic, complete unilateral cleft lip and palate. Initial outcomes of interest were dental arch alignment, midfacial growth and facial profile, and nasolabial esthetics. Follow-up studies also considered orthognathic outcomes at skeletal maturity, speech, burden of care, and patient satisfaction. Results are summarized in Table 1 but highlighted much disparity in protocols and outcomes between centers. Results of the Eurocleft studies kindled a desire for quality improvement in the cleft-care community at large. With funding from the European Union, a registry of European cleft teams was created. It issued a policy statement that delineated practice guidelines for the treatment of children with clefts and that recommended minimum recordkeeping standards for teams. EUROCRAN was conceived to help organize clinical and genetic research and to foster collaboration. Many of the Eurocleft researchers also participated in the World Health Organization’s (WHO) development of an international strategy to craniofacial research, bringing Eurocleft’s quality-improvement aims to a worldwide audience.
| Patient Characteristics | No. of Centers | Location(s) | Measures Reported | ||
|---|---|---|---|---|---|
| Cleft Type | Age at Evaluation | No. Enrolled | |||
| Eurocleft | |||||
| cUCLP | 8–10 | 151 | 6 | UK, Sweden, Denmark, Netherlands, Norway | Craniofacial form (cephalometry) |
| 11–14 | 131 | 6 | Dental arch relationships (GOSLON) | ||
| 12, 17 | 124 | 5 | Nasolabial appearance (Asher-McDade scale) | ||
| Speech (structured, multilingual) | |||||
| Burden of care | |||||
| Craniofacial form (cephalometry) | |||||
| Dental arch relationships (GOSLON) | |||||
| Nasolabial appearance (Asher-McDade scale) | |||||
| Patient/parent satisfaction questionnaire | |||||
| CSAG | |||||
| cUCLP | 5, 12 | 457 | 50 | UK | Craniofacial form (cephalometry) |
| Dental arch relationships (5-year-old index, GOSLON) | |||||
| Success of alveolar bone grafting (modified Bergland) | |||||
| Nasolabial appearance (Asher-McDade scale) | |||||
| Patient/parent satisfaction questionnaire | |||||
| Speech (modifed CAPS) | |||||
| Americleft | |||||
| cUCLP | 6–12 | 172 | 5 | US, Canada | Craniofacial form (cephalometry) |
| Dental arch relationships (GOSLON) | |||||
| Nasolabial appearance (Asher-McDade scale) | |||||
| Speech (pending) | |||||
| Scandcleft | |||||
| cUCLP | 5 | 445 | 10 | Denmark, Sweden, Finland, Norway, UK | Craniofacial form (cephalometry) |
| Dental arch relationships (5-year-old index) | |||||
| Nasolabial appearance (Asher-McDade scale) | |||||
| Speech (structured, multilingual, nasometry) | |||||
In response to poor outcomes obtained by British centers participating in the Eurocleft studies, the Clinical Standards Advisory Group (CSAG) performed an audit of all 5- and 12-year-old children in the United Kingdom with unilateral cleft lip and palate. Results were poor across all measures (see Table 1 ). CSAG proposed specific methods for restructuring the cleft-care-delivery process and created specific service specifications for providers. Based on these findings and recommendations, the National Health Service made reorganization of cleft-care services a national priority in 1999, a process that was completed in 2005. A key principle established when cleft services were centralized in the United Kingdom was that results should be routinely collected and assessed. A national database, CRANE, was set up ( https://www.crane-database.org.uk/ ); use of electronic databases in individual units was made the norm, and the Craniofacial Society of Great Britain and Ireland (CFSGBI) set out an agreed minimum dataset for audit. Recently, a follow-up cross-sectional study, Cleft Care UK, was begun to monitor improvement in outcomes of 5-year-old children treated following the reorganization of services.
Inspired by the success of the Eurocleft project, the ACPA convened a taskforce in 2006 to establish a similar multicenter collaborative effort in North America. Named Americleft, the 5 participating centers compared outcomes using existing clinical records and the methodology described in the Eurocleft studies. Results are summarized in Table 1 .
The rich history of collaborative research in cleft care underscores the complexity and considerable difficulty inherent in retrospective comparisons of outcomes from diverse institutions. These studies also demonstrate the great potential of multicenter collaborations. Presently, new collaborations are underway in Scandinavia, Japan, India, Brazil, and Australia. In particular, the 10-center Scandcleft collaborative has progressed beyond retrospective observational studies to use randomized controlled trials for the evaluation of surgical technique, timing of individual interventions, and sequence of interventions (see Table 1 ). The planning and execution of prospective research methods mark a significant advance in cleft research.
Conceptualizing outcomes in cleft care
What to Measure in Cleft Outcomes?
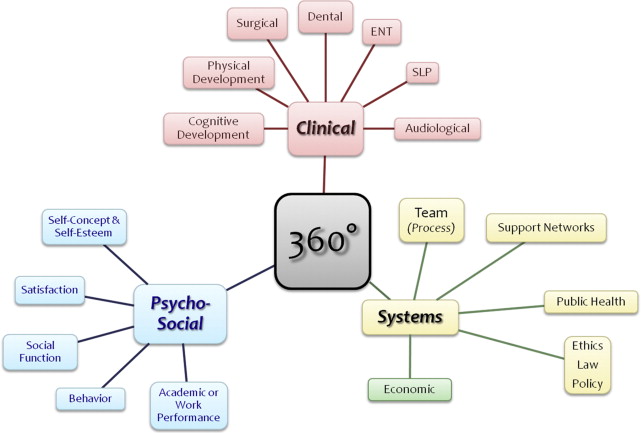
From a holistic perspective, the patient should be conceptualized as the center of the health care delivery process ( Fig. 1 ). Three principal domains for outcomes are clinical, psychosocial, and systems-based parameters. The clinical domain includes aspects common to traditional clinical outcomes studies and includes many subdomains such as general pediatrics (eg, physical and cognitive development), surgery, dental/orthodontic, speech, and audiology. The psychosocial domain is arguably equally important and includes aspects related to psychological well-being and social functioning. Some psychosocial elements may be intricately related to traditional clinical outcomes; for example, self-perception of appearance may be related to nasolabial appearance, and academic performance may be related to cognitive development. However, these qualitative elements carry the additional semantic value of “how does this matter to the patient?” missing from traditional quantitative clinical outcomes. A third domain in the conceptualization of outcomes in cleft care is systems-based parameters . These elements may pertain to cost, resource allocation, process of care (eg, efficiency), supplemental/ancillary services, and so on and are typically used in value assessments and continuous quality improvement endeavors.