57 Maximizing Graft Survival in Follicular Unit Excision: The Implantation Phase
Summary
Keywords: graft placement graft implantation follicle splay follicle skeletonization forceps implantation graft implanters repetitive placement trauma
Key Points
•The success of follicular unit excision (FUE) is greatly influenced by the graft placement technique.
•Implanters are the best placement technique for FUE grafts with splay and bare follicles.
•The forceps placement technique must be modified for FUE grafts.
57.1 Introduction
Follicular unit excision (FUE) surgery is comprised of two steps, graft excision and graft implantation. The first step, graft excision consists of two phases (graft incision and graft extraction), which are discussed in Chapter 56. The second step, graft implantation, is one of the most important phases of hair restoration surgery. Trauma during this phase is a common cause of poor growth. Dr. Bradley R. Wolf discusses graft implantation in detail in Chapter 45 of this textbook as well as in his excellent article in Hair Transplant Forum International.1
It is widely recognized that graft placement during FUE surgery is more difficult, and presents unique challenges, not present with strip-FUT. Whereas all the technical considerations that apply to graft placement with strip surgery apply to FUE, there are some extra challenges that present when placing grafts with FUE.
In the past, comparison studies on survival have shown yield in FUE to be less than FUT.2 The cause of this lower yield with FUE was felt to be due to multiple factors intrinsic to the FUE process. One factor was attributed to injury caused by excessive force during the graft extraction (pulling) phase that crushes or tears follicles. Another factor is that FUE grafts have characteristics that make them difficult to place without injury. These include skeletonized or denuded grafts, exaggeration of follicle splay, the absence of “safe” tissue to grasp with forceps, and greater vulnerability to desiccation.
A few more recent studies, using some of the advancements in FUE technology, have suggested that yield with FUE can be equal to (or even greater than) FUT when these characteristics are addressed and mitigated.2,3 Special techniques, care, and attention are required in FUE graft handling and placing to get maximum yield.
57.2 Preserving Graft Quality During the Excision Phase
The focus of this chapter is on graft preservation during the implantation phase, but it is worthwhile to review important aspects of the excision phase that have a direct negative effect on survival during the implantation phase.
57.2.1 Preventing Skeletonized Grafts
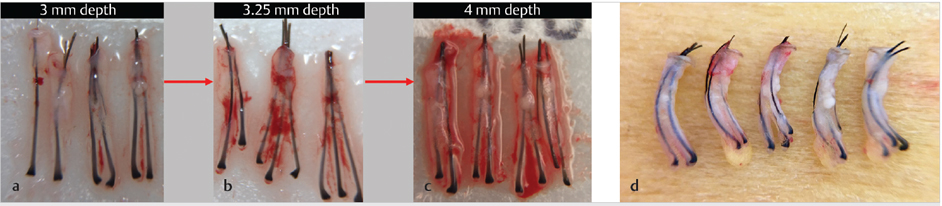
Skeletonized grafts are stripped of perifollicular tissue in the lower portion of the graft (Fig. 57.1). In the extreme, only the upper third of the graft will have perifollicular tissue. Studies by Beehner5 support the observation that “chubby” grafts survive better than “skinny” grafts that have no cutaneous tissue around the follicles. The exact mechanism for this is not proven, but it is widely believed that grafts stripped of tissue are both more easily desiccated and traumatized during extraction and placement. Skeletonization is largely a consequence of a too shallow punch insertion. If at any point during an FUE surgery grafts are seen to be skeletonized, the punch depth should be set deeper until the skeletonization is minimized (Fig. 57.2a–c). There is a delicate balance in judging how deep to go because there is a point at which, particularly with sharp punches, deeper punch penetration will increase follicle transections. Blunt and newer “hybrid” punches typically allow deeper penetration without increasing transections and therefore minimize skeletonization, creating grafts more similar to FUT grafts (Fig. 57.2d). In 2018, Josephitis and Shapiro presented a side-by-side study on the same patient comparing survival of FUE versus FUT grafts. The FUE grafts in this case were obtained with the newer hybrid punch technology, and therefore had more perifollicular tissue surroundings their base. They looked similar to the FUT grafts. The survival was basically the same for FUE and FUT, using cross-section trichometry (CST; HairCheck) and hair counts as study parameters.3
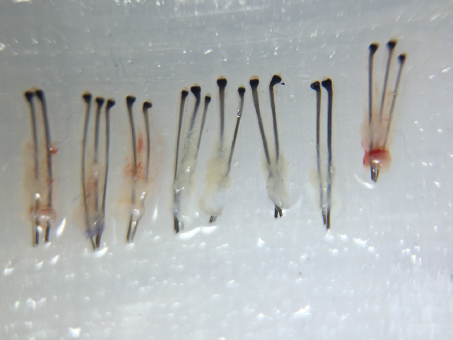
Fig. 57.1 Skeletonized graft.
57.2.2 Minimizing Follicle Splay
Follicular splay is the term used to describe a follicle (or all follicles within a graft) that diverges outward and away from adjacent follicles (Fig. 57.3a).6,7,8 Splay typically occurs in the proximal portion (lower one-third) of the follicular unit and can vary in degree. Dr. True has recently introduced the concept of structural splay and iatrogenic splay. Structural splay exists anatomically in the tissue and varies both among patients and within the same patient (Fig. 57.3b). Iatrogenic splay is splay produced when the FUE punch incision depth has not been adequate to overcome the tissue tethering forces during extraction. FUE techniques in which the punch is inserted superficially may often produce extreme splay of the bulb portion of the follicles as a consequence of stripping way the perifollicular tissue during the extraction phase of excision (Fig. 57.3c). Splayed grafts are very difficult to place with forceps and are more amenable to implanter placement. Graft quality problems such as skeletonization typically accompany iatrogenic splay. Dull punches and newer hybrid punches minimize splay because they allow the punch to go deeper with less risk of transection.
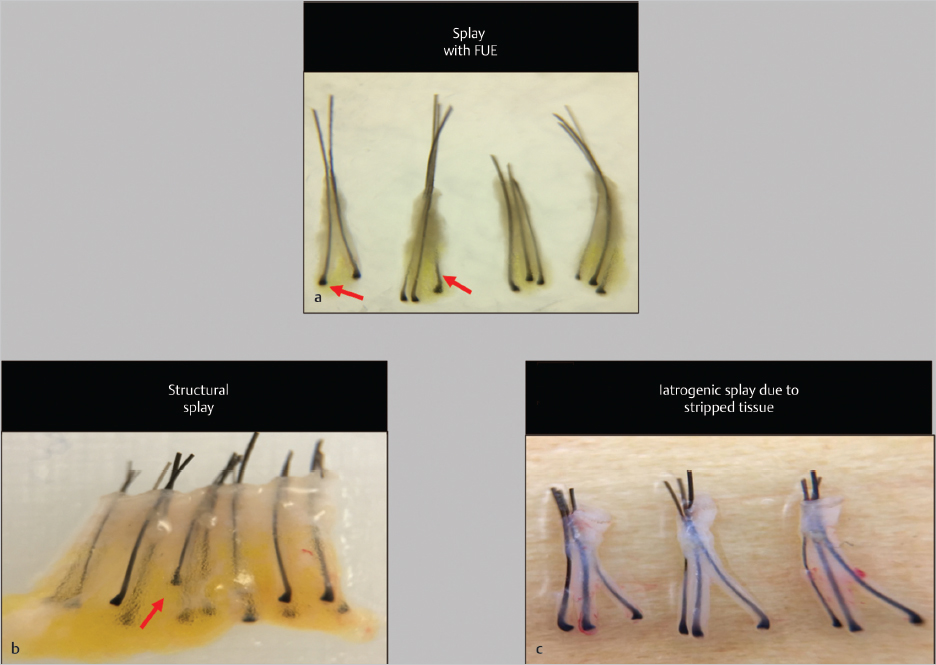
Fig. 57.3 (a) Splay showing follicles directed away from each other in the lower third. (b) Example of structural splay and variable splay in the same person. (c) Iatrogenic splay from stripped tissue.
57.3 Avoiding Graft Damage During Placement
57.3.1 Trauma During Graft Implantation
•Repetitive placement trauma (RPT)1 is a term coined by Dr. Wolf. (Dr. Ron Shapiro also called this phenomenon “multiple failed attempts” in the 2004 edition of this textbook). When grafts are repeatedly handled during failed implantation attempts, the risk of graft damage and poor yield is increased.
•Crush injury, caused by squeezing the bulb too forcefully with forceps, is another cause of graft injury.
•Bent grafts (curved grafts, J-hook rafts) are a recently described entity that seems to be associated with decreased yield (and perhaps folliculitis or kinky growth). This is felt to be caused by one leg of a graft getting caught on the edge of an incision, or forceful jamming of a graft into an incision during placing (Fig. 57.4).

Fig. 57.4 Bent or “J” hair trauma.
Related posts:
 The Patient with Minimal Hair Loss: Planning and Decision-Making
The Patient with Minimal Hair Loss: Planning and Decision-Making
 Hair Anatomy and Histology for the Hair Transplant Surgeon
Hair Anatomy and Histology for the Hair Transplant Surgeon
 Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
Plugged in: How to Ensure That Your Practice Thrives (and Survives) in Today’s DigitalWorld
 Transplanting into Areas of Cicatricial Alopecia
Transplanting into Areas of Cicatricial Alopecia
 Special Considerations for Postoperative Care in Follicular Unit Excision
Special Considerations for Postoperative Care in Follicular Unit Excision
 Hairline and Recipient Area Repair of Poor Previous Transplantation
Hairline and Recipient Area Repair of Poor Previous Transplantation
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


