Mammography in a patient with prior silicone injection: multiple bilateral dense nodular images corresponding to siliconomas, which prevent the evaluation of underlying parenchyma. (Courtesy of Dr. Román Rostagno)
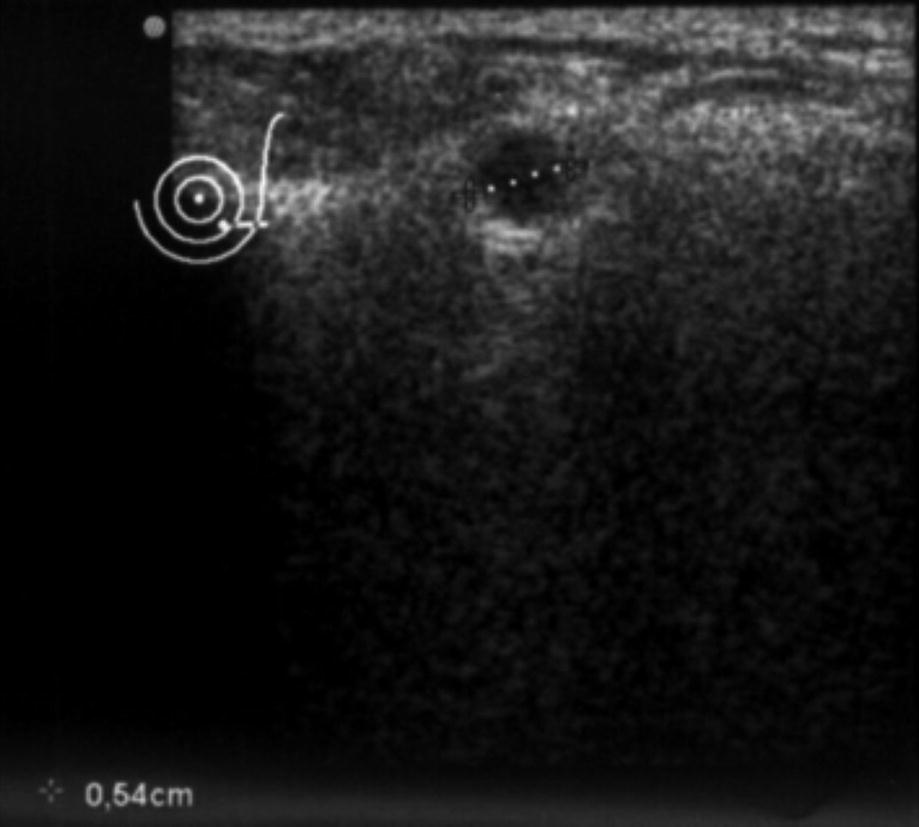
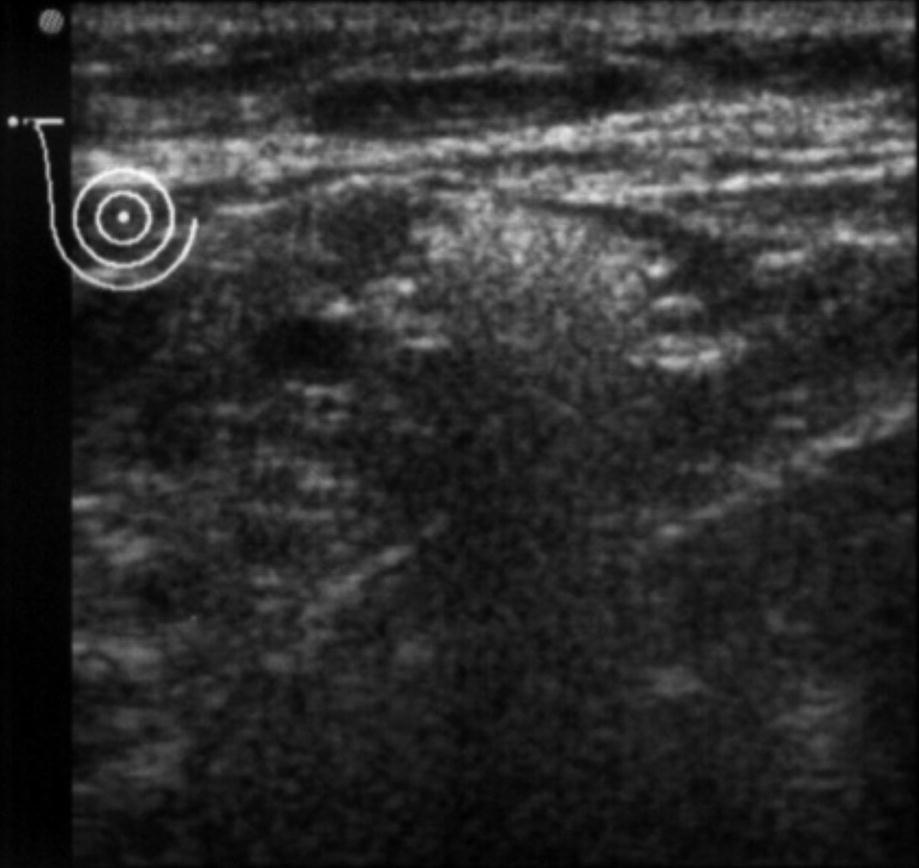
Ultrasound reveals siliconoma nodules and the classic “snowstorm” appearance. (Courtesy of Dr. Román Rostagno)
Ultrasound reveals axillary lymph node infiltration by silicone within the hilum. (Courtesy of Dr. Román Rostagno)
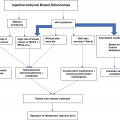
Macronodular
Micronodular
Mixed
Snowstorm appearance
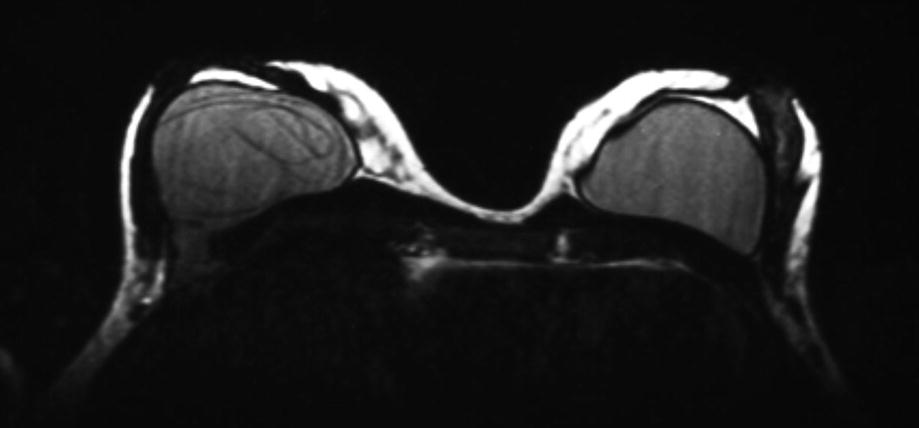
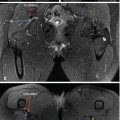
Magnetic resonance imaging (MRI) demonstrates both intracapsular and extracapsular prosthesis rupture and silicone leakage. (Courtesy of Dr. Román Rostagno)
The F-FDG PET/CT study used to track breast cancers has no use in silicone-injected patients, since it has an unacceptably high false-positive rate for breast cancer [10, 11], as well as for axillary adenopathy [12].
The Therapeutic Plan
In their algorithm, Liu et al. [13] describe two fundamental parameters that define therapeutic choices: the state of the teguments that cover the breast and the extent of siliconomas. As it is not surgery for cancer, the surgeon’s obligation is to conserve the nipple-areola complex in situ, if feasible. The plan, always surgical, is usually inclined toward combining “simile” subcutaneous adenomastectomy and immediate reconstruction – since the lesions generally are diffuse and attempts to reduce the extent of surgery increase the likelihood that granulomas will be left behind. The addition of “simile” means the little that it has of true “subcutaneous adenomastectomy” that resects “all” the gland to leave only the adipose tissue between Cooper’s ligaments and the skin. In my experience with this type of surgery for patients with mammary siliconomas caused by injection, achieving subcutaneous adenomastectomy “by the book” is impossible and even dangerous, due to the likelihood of postoperative tissue sloughing. With these clarifications, all the possibilities are exposed.
Partial Mastectomy
Whether with or without symptoms, it is rare for a patient to present to surgeons with breast disease that is restricted to a single sector or quadrant of the breast and no evidence of silicone outside the area. If it is necessary to use local flaps, these must be undamaged. This is the only case in which a surgeon can resect the affected area and perform direct closure without having to resort to flaps, the least, both glandular of the breast itself or with the help of the latissimus dorsi. Echo et al. [14] reported that, of their 14 female patients who underwent surgery for mammary pathology produced by silicone injections, only 2 were treated with local resection and mammary parenchymal flaps.
Subcutaneous Adenomastectomy
Subcutaneous adenomastectomy allows for the resection of all glandular tissue – with the exceptions exposed – and conservation of the areola-nipple complex. For this procedure to be viable, it is essential that the skin covering the breast is undamaged, which happens in a minority of patients, since most present with advanced pathologies that have already compromised the skin. If involvement is limited to one sector – most conveniently the lower sector – incisions can be adapted to allow the skin to be resected and, from there, completion of the adenomastectomy.
It is essential to remember that this surgical approach is difficult to execute, since the ablation of all glandular tissue is never safe. The more you want to limit the dissection that occurs between the glandular plane and the adipose tissue that interposes between it and the skin, the greater the patient’s risk of postoperative skin necrosis. In general, one should leave a thickness not less than 1 cm for the teguments, knowing that some siliconomas often remain after surgery and reconstruction is intended. Chiu et al. [15] used this technique bilaterally in five patients, with a peri-areolar incision, inverted “T,” or inframammary plus bilateral TRAM reconstruction.
Total Mastectomy with Nipple and Areolar Preservation
Although the overriding goal of surgery, similar to that described in the previous paragraph, is to resect the largest amount of mammary gland tissue, this technique resects more affected skin. It also requires that the areola-nipple complex be intact and that imaging studies exhibit no evidence of siliconomas immediately below the nipple-areolar complex. Otherwise, attempts to preserve the nipple and areola create the risk that both eventually will slough off.
Total Mastectomy with Nipple and Areola Resection
This is the surgical option that is warranted when there are glandular deformities and involvement of the skin, occasionally including the nipple-areolar complex in advanced disease. When the indication for this surgery is not cancer, the aponeurosis of the pectoralis major muscle may be preserved. At other times, among patients in whom the entire mammary gland is filled with siliconomas, adhered to the aponeurosis secondary to chronic inflammation, whether ultrasound reveals a nodular or diffuse (snowstorm) appearance, it is preferable to include it in the resection piece to avoid leaving residual siliconomas in intimate contact with the aponeurosis. Whether this type of breast reconstruction is performed, or not, is typically at the discretion of the plastic surgery team.
Axillary Exploration, Plus/Minus Total Resection
To delineate the extent of the siliconomas: breast alone, versus breast and axilla, versus even more extensive spread
To rule out otherwise hidden carcinoma
To provide further confirmatory evidence that no cancer is present, when confidence in a negative percutaneous biopsy is low, due to diffuse siliconomas
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


