(a, b) Siliconomas. Typical mammography and ultrasound with a “snowstorm” image
Preoperative Planning
Measuring the base and height of the breast
As with all surgical procedures we perform for breast reconstruction or remodeling after a wide local excision, our strategy begins with a careful preoperative evaluation. With the patient standing in front of us, we first mark the position of what will become the new nipple-areola complex, with a vertical T between 5 cm and 7 cm in length.
Surgical Procedure

De-epithelization of the lower area of the skin between the breast groove and the medial and lateral extensions of the reduction pattern
Before the mastectomy is started, the skin incisions are marked to the submammary groove, as we seek to perform its careful anatomical preservation. The gland must be resected, with precise preservation of the subdermal vascular network of the upper and lateral flaps. We always tend to dissect in the plane of Cooper’s ligaments, to minimize ischemia without compromising complete removal of breast tissue.

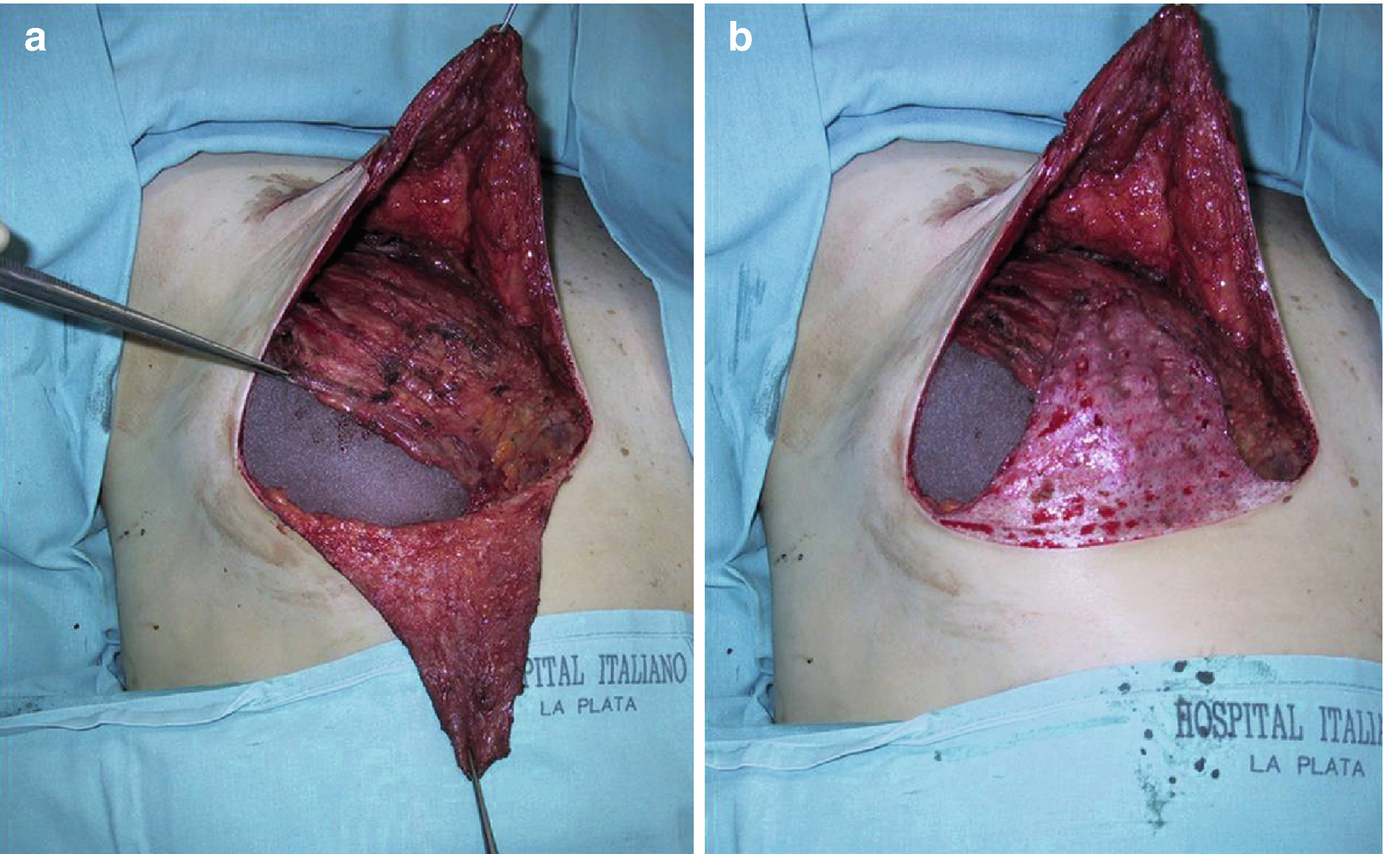
(a, b) Appearance of the dermal-fat flap before pectoralis major muscle detachment
In women with gigantomastia and more than a 4 cm distance to the new mobilization point, the nipple-areola complex is reconstructed in a second stage under local anesthesia. In selected patients, this autograft can be performed, even if it is not clear whether the superior flap can provide adequate vascularization. In some cases, the nipple can be reconstructed during the first operation with local skin flaps.
Discussion

Dermal-fat flap, before pectoralis major detachment
Using the combined pocket, we have had the opportunity to place large mammary implants (average volume 400 cm3). The wide upper access has afforded us the potential to identify the lymph nodes in all cases and avoid a second scar in the axilla. Even axillary dissection, in the vast majority of cases (85%), can be performed through this access route. However, it is advisable to avoid traction to prevent damaging the flaps’ vascular supply.
One aesthetic advantage of this mastectomy technique with cutaneous reduction is that patients with medium or large breasts benefit from simultaneous bilateral reduction and attain a symmetrical result.
With this technique, we have observed a 13% rate of serious complications — requiring implant removal — and an overall complication rate of 20% (mostly superficial epidermolysis or wound dehiscence).
In our series, 75% of the implants removed were from patients who smoked more than 20 cigarettes per day. Some authors suggest evaluating the viability of the skin with fluorescein to detect ischemia intraoperatively, as recommended by Carlson et al. [3] We, however, have not found this approach to be useful. Instead, we base our evaluation solely on clinical observation of flap skin color and the redness of the blood at the wound edges. A third of all our complications can be managed effectively with conservative treatment, while the other two thirds progress to exposing the implant. Catecholamine released as an effect of nicotine damages skin vascularity, particularly the thin, long skin strips of the flaps [3]. Carlson et al. linked tobacco consumption to a significantly higher rate of necrosis in a subset of smokers who underwent a skin-sparing mastectomy (49% vs. 19% rate of necrosis in the non-smoking group). We advise that surgeons avoid using the technique described above in heavy smokers and patients with microvascular disorders (e.g., diabetes, radiotherapy). In our opinion, the technique’s complication rate can be reduced by judicious selection of patients and should decline as surgeons gain more experience.
Although the latissimus dorsi flap plays an important role in the repair of reconstructions that fail, due to extensive necrosis of the skin, we have never used it as a salvage flap. In all our complicated cases, the skin flaps were still wide enough to allow for placement of an expander and conversion to a conventional two-stage procedure.
Capsular contracture is one of the main problems observed with reconstructions involving implants, in terms of altering the new breast’s final appearance. All our patients were classified as having either a grade I or II Baker’s contracture (median follow-up, 13.6 months). In our opinion, complete release of the pectoralis major muscle and the double fat-skin plane allowed for very smooth and natural reconstruction.
Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


