Masseter-to-Facial Nerve Transfer
Michael J. A. Klebuc
DEFINITION
The descending branch of the masseter nerve can be transferred to selected zygomatic-buccal branches of the facial nerve (V-VII) to restore motion in the midface and perioral region.
The V to VII nerve transfer is utilized when intracranial and/or intratemporal segments of the facial nerve are irreversibly damaged in the presence of intact distal facial nerve branches and viable muscles of facial expression.
ANATOMY
The masseter nerve branches from the mandibular nerve and passes above the lateral pterygoid muscle where it runs through the mandibular notch to enter the substance of the masseter muscle.
Along its intramuscular path, the main trunk liberates a series of small proximal branches and terminates in a long descending branch that courses obliquely in a posterioranterior, proximal-distal trajectory.
The main trunk of the masseter nerve can be identified at a point 3 cm in front of the tragus, 1 cm below the zygomatic arch, and 1.5 cm deep to the SMAS (FIG 1).1
The masseter muscle has three lobes (superficial, middle, and deep).
The motor nerve to masseter (CN V) lies on the superficial surface of the deep lobe.2
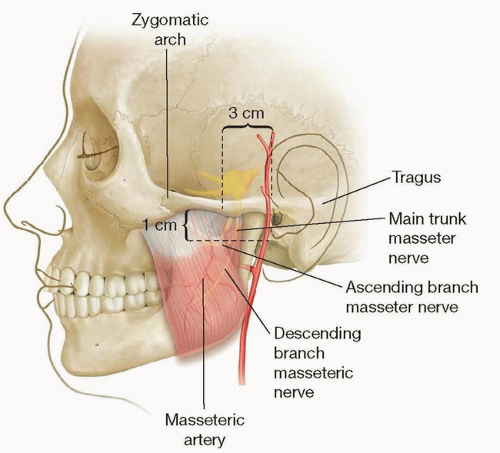
FIG 1 • Topographic landmarks for isolation of the motor nerve branch to masseter. The main trunk is identified 3 cm in front of the tragus, 1 cm below the zygomatic arch, and 1.5 cm deep to the SMAS.
The main trunk and descending branches contain approximately 2700 and 1550 myelinated motor fibers, respectively.1,3
The descending branch of the masseter nerve is usually selected for the V to VII transfer.
Facial nerve (somatic motor efferent component) innervates the muscles of facial expression, auricular muscles, occipitalis, posterior belly digastric, stylohyoid, and stapedius.
The facial nerve main trunk emerges from the skull base via the stylomastoid foramen where it can be identified coursing 1 cm deep to the tragal pointer and medial to the posterior belly of the digastric muscle.4
Within the parotid gland, the facial nerve divides into a temporofacial and cervicofacial trunk.
Distal branches exit the parotid along its anteromedial border.
The following branches innervate the corresponding muscles of facial expression5:
Frontal branch—frontalis muscle
Zygomatic branches—orbicularis oculi, zygomaticus major, zygomaticus minor, levator labii superioris, levator labii superioris alaeque nasi, corrugator supercilii, procerus
Buccal branches—buccinator, risorius, orbicularis oris
Marginal mandibular branches—depressor anguli oris, depressor labii inferioris, mentalis
Cervical branches—platysma
Zuker point-midway point of a line drawn from the root of the helix to the lateral commissure (FIG 2)6:
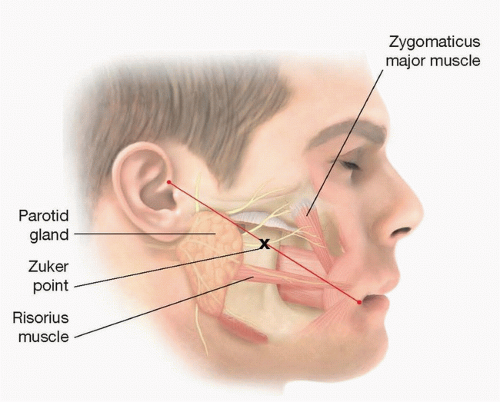
FIG 2 • The facial nerve branch supplying the zygomatic major is typically found at a point half way between the root of the helix and the lateral commissure.
Describes the approximate location of the facial nerve branch supplying the zygomaticus major muscle.
At this location, the zygomatic facial nerve branches coursing above and below the transverse facial artery are often selected for the V to VII transfer.
PATHOGENESIS
Employed when intracranial and/or intratemporal segments of the facial nerve are irreversibly damaged in the presence of intact distal facial nerve branches and viable mimetic muscles.
Commonly utilized after ablative oncologic surgery or trauma involving the brainstem and skull base.
Etiology of facial nerve injury includes resection of acoustic neuroma, facial nerve schwannoma, cerebellopontine angle tumors, AVM, cholesteatoma, and skull base tumors. Unrecovered Bell palsy, mastoiditis, and skull base fractures are other common causes of facial nerve injury.7
PATIENT HISTORY AND PHYSICAL FINDINGS
The duration of the paralysis is one of the most important pieces of information garnered from the patient’s history, as the masseter-to-facial nerve transfer must be performed before the muscles of facial expression have undergone irreversible atrophy.
The V to VII transfer is optimally employed immediately at the time of tumor extirpation yet remains a viable option up to 18 months after the onset of the paralysis.
The patient’s age is also of consequence in surgical planning. Generally, in the older patient population (greater than 55 years), the V to VII transfer is used in isolation with fascia lata grafts for additional static support. In younger patients, the V to VII transfer is often combined with cross face nerve grafts (CFNG) in a single operative setting. This is performed in an effort to create a marriage of power (V-VII) and spontaneity (CFNG).8,9
A history of diabetes, coronary artery disease, chronic obstructive pulmonary disease, smoking, underlying neurologic disorders, previous head-neck radiation, and temporal mandibular joint dysfunction should be noted and accounted.
The patient’s level of motivation and willingness to comply with postoperative physical therapy is also important to ascertain.
On physical examination, active, forceful contraction of the masseter and temporalis muscles is confirmed by palpation.
The face is examined for previous access incisions and signs of trauma or injury to the muscles of facial expression.
Dental occlusion and mouth opening are evaluated to rule out temporomandibular joint dysfunction.
A cranial nerve examination is performed to identify additional neurologic deficits.
The eye is examined for signs of exposure keratitis as adjunctive eye procedures may be performed with the V to VII transfer to maintain corneal health.
A vascular examination of the lower extremities is undertaken to rule out significant peripheral vascular disease if fascia lata or sural nerve grafts are to be harvested.
IMAGING
MRI of the brain and facial nerve
High-resolution multiplanar T1 and T2 images, gadolinium enhanced, fat suppressed, and internal auditory canal (IAC) protocol
Used to evaluate injury to the facial nerve (ie, Bell palsy, tumors, stroke)
Computed tomography
0.625 mm or thinner axial images, reconstructions in coronal plane
Valuable for imaging temporal bone fractures
EMG of the masseter muscle and mimetic muscles innervated by the facial nerve
Look for signs of early facial nerve recovery.
Look for signs of reversible muscle atrophy.
Look for signs of coordinated activity between the mimetic muscles and the masseter.
SURGICAL MANAGEMENT
Preoperative Planning
Smoking cessation and avoidance of nicotine
Discontinuation of oral anticoagulants
Facial nerve imaging as guided by the etiology of the paralysis (MRI, CT)
EMG
Presence of muscle fibrillation (suggests potential, positive response to reinnervation)
Concomitant activation of the masseter muscle with smiling (may predict development of an effortless smile)
Positioning
Supine on the operating table with arms tucked
Narrow head extension with foam or gel-filled headrest
Nasotracheal intubation with nasal RAE endotracheal tube sutured to the columella and supported on the hair-bearing scalp with foam, silk tape, and staples (FIG 3)
Oral cavity cleansed with chlorhexidine gluconate mouthwash
Lower extremities prepped if nerve or fascia grafts are to be utilized

FIG 3 • Nasotracheal intubation with head positioned on a narrow headrest. Endotracheal tube sutured to columella and supported with foam to prevent pressure on the nasal alae.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access