Mandible Reconstruction With Fibula Free Flap Using CAD/CAM Techniques
Jamie P. Levine
David L. Hirsch
Lawrence E. Brecht
DEFINITION
Recent advances in imaging, computer-aided design/computer-aided modeling (CAD/CAM) software, and 3D printing technology have enabled virtual planning of complex 3D osseous reconstruction of head and neck defects.1,2,3,4,5
Using these methods, we can now prepare exact models and customized surgical devices that facilitate and simplify reconstruction. Virtual surgical planning and customized surgical templates decrease the learning curve for osseous reconstruction of head and neck defects while simultaneously improving the precision of reconstruction.6
This is important because traditional methods for surgical planning of these reconstructions have a steep learning curve and even small errors can lead to poor outcomes.
CAD/CAM virtual surgical planning also increases collaboration with oncologic and dental colleagues leading to a more unified plan. This approach allows development of more creative solutions for complex defects that ordinarily would be difficult to visualize preoperatively.7,8
This chapter will provide step-by-step planning for mandible reconstruction using the fibula flap with CAD/CAM planning. This approach can easily be modified for use with other osseous sources (eg, iliac crest, scapula, etc.) or for reconstruction of other osseous defects of the head and neck (eg, maxilla).
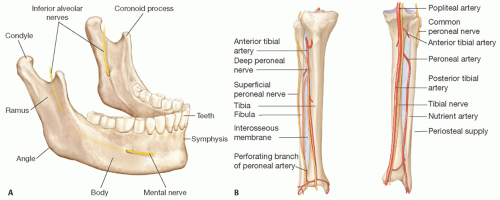 FIG 1 • A. Anatomy of the mandible. B. Anatomy of fibula flap. |
ANATOMY
Mandible
The mandible is a complex 3D structure with two symmetric points of articulation at the skull base forming the temporomandibular joint (FIG 1A).
The mandibular body and the curved mental protuberance contain 16 sockets to hold the lower teeth. The ramus and condyle form the articulation points with the skull base.
The mandible has two foramina.
The mandibular foramen is located on the internal surface of the ramus and serves as the entry point for the inferior alveolar nerve.
The mental foramen is on the external surface of the mandibular body, below the second premolar. The inferior alveolar nerve exits the mandibular canal at this location and then becomes the mental nerve.
The mandible serves as the attachment point for multiple muscles, including the muscles of mastication that help coordinate movement of the mandible with chewing.
The blood supply of the central mandible is derived from multiple sources including the inferior alveolar artery and periosteal branches from the surrounding musculature.
Fibula flap
The fibula is the preferred choice for mandible reconstruction in most patients7,9 because of the following characteristics: the bone has a dual blood supply (periosteal and axial) enabling complex shaping of the bone; there is a large amount of bone available (20-25 cm) enabling reconstruction of subtotal mandibulectomy defects; the vascular supply is consistent and large caliber; the bone stock is sufficient for dental rehabilitation; and finally, because the fibula can be harvested simultaneously with the oncologic resection.
The dual blood supply of the fibula enables surgeons to perform multiple osteotomies to achieve the complex shape of the mandible. However, in general, segments are planned.
The blood supply for the fibula is derived from the peroneal artery and vein (FIG 1B).
The pedicle length is variable and depends primarily on the amount of bone that is needed and anatomic variability in the take off of the peroneal artery/vein from the tibioperoneal trunk. In general, the length of the pedicle can be planned preoperatively using virtual surgical planning and angiography.
PATHOGENESIS
CAD/CAM virtual surgical planning can be used for acquired and congenital defects of the mandible. The most common cause of mandibular defects necessitating vascularized bone transfer is oncologic resection of the mandible for malignant tumors (FIG 2).
These tumors include primary bone tumors (eg, osteogenic sarcoma) or more commonly, metastatic spread from squamous cell cancer of the soft tissues of the head and neck (eg, floor of mouth or tongue).
Osteoradionecrosis is a common complication of radiation therapy of the head and neck and in some cases results in late defects of the mandible. These patients present with nonhealing wounds or pathologic fractures of the mandible and in some cases, benefit from resection of the necrotic bone and reconstruction with free flaps.
Benign lesions such as ameloblastoma, giant cell tumors, odontogenic mandibular cysts, and odontogenic tumors (ie, ameloblastoma) also require resection and reconstruction. These lesions do not metastasize but can be locally aggressive and have a high risk of recurrence if not resected with appropriate margins.
Traumatic injuries, and less commonly infectious etiologies (eg, refractory osteomyelitis), resulting in bone loss or complex lesions with nonunions also require osseous reconstruction in select cases.
Congenital defects of the mandible in rare cases require free tissue transfer with bone flaps. More commonly, these defects are treated with bone grafting or distraction osteogenesis.
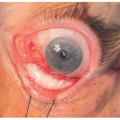
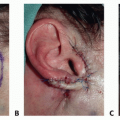
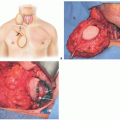
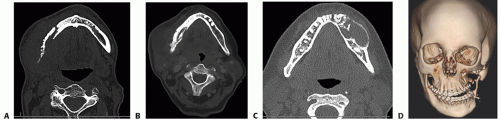 FIG 2 • Common causes of mandibular defects. A. Right mandibular osteoradionecrosis with surrounding infection. B. Squamous cell carcinoma of the right hemimandible. C. Left mandibular ameloblastoma. D. Treacher Collins syndrome with resorbing left mandibular rib graft. |
PATIENT HISTORY AND PHYSICAL FINDINGS
The history and findings will depend mainly on the cause of disease process.
For all patients, bone donor sites should be carefully assessed for blood supply, quality of soft tissues, and bone stock.
Similarly, the anticipated defect in the mandible should be assessed for osseous and soft tissue needs and recipient vessels for microsurgery. Mouth opening, mastication, and swallowing should be examined.
The quality and quantity of the teeth should be assessed and dental consultation should be obtained as needed.
Dental rehabilitation (bone implants at the time of surgery or in a delayed fashion versus dentures) should be considered if feasible and discussed with the dental team.
Medical comorbidities, prior treatments, planned treatments postoperatively, and prognosis should be assessed and noted whenever feasible.
Patients with osteoradionecrosis or osteomyelitis may need to be optimized for treatment preoperatively using hyperbaric oxygen treatment, debridement, and antibiotic treatment as needed.
IMAGING
Fine cut (1-mm-thick sections) CT scans of the mandible and fibula with 3D reconstruction is the best option for examining the bone and for planning of the reconstruction. MR imaging may also be useful in some cases to evaluate the surrounding soft tissues but is not useful for developing 3D bone models (FIG 3).1,2
The mandibular CT scan is usually performed as a noncontrast study because the primary need is to evaluate the bone anatomy and anticipated defects.
Imaging of the fibula flap is typically done with a CT angiogram to evaluate the osseous anatomy as well as the vascular blood supply. The angiogram is used to evaluate the vascular anatomy of the lower extremity (three vessel runoff, abnormal vascular anatomy), and the perforator anatomy of the skin paddle. This imaging helps with planning the placement of the osteotomies and skin paddles.
Although standard models of the fibula are available and may be used for planning, in our hands, CT scans of the patient’s own fibula is more accurate since because is some variability in the shape of the bone that may alter the angles needed for shaping of the fibula.
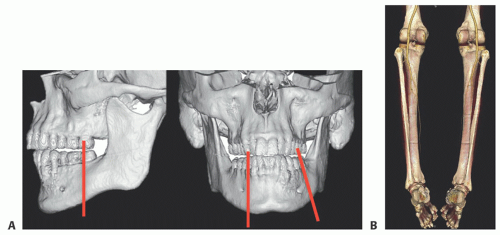 FIG 3 • A. Three-dimensional model of the mandible derived from thin cut CT scans demonstrating area to be resected (red bars). B. CT angiogram of the lower extremity and fibula anatomy. |
 FIG 4 A. Virtual surgical planning and design of mandibular (left) and fibula (right) cutting guides. B. Top-down plan for mandible reconstruction. Double barrel fibula flap reconstruction is planned with positioning of the mandibular segment along the upper border of the mandible to facilitate dental implant placement. C. Fibula cutting guide with predictive holes for placement of prebent plates and positioning of double barrel segment. D. Final placement of dental implants with double barrel fibula flap reconstruction. |
SURGICAL MANAGEMENT
Preoperative Planning
The CT scans of the mandible and fibula are used for preoperative virtual surgical planning with the oncologic surgeons, dentists (if necessary), and the reconstructive team.
It is important for the ablative surgeon to be involved in the planning session to accurately plan surgical margins. In cases where there is doubt about the surgical margins, two separate plans can be prepared. This approach enables intraoperative modification of the virtual surgical
plan depending on anatomic or oncologic findings. Thus, a “narrow” margin resection plan may be created as the initial plan; however, if intraoperative findings dictate larger resection, then the backup “wider” resection plan can be executed instead. This approach creates two separate cutting guides for the head and neck and fibula harvest plans (FIG 4A).Related posts:
 Mandible Reconstruction With Fibula Flap With Templates
Mandible Reconstruction With Fibula Flap With Templates
 Repair of Lip Defects With Karapandzic Flaps
Repair of Lip Defects With Karapandzic Flaps
 Lower Eyelid Reconstruction With Palatal Grafts
Lower Eyelid Reconstruction With Palatal Grafts
 Reconstruction of the Ear Lobe
Reconstruction of the Ear Lobe
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


