Mandible Reconstruction With Fibula Flap With Templates
Eric G. Halvorson
DEFINITION
Mandible reconstruction is most commonly indicated following tumor extirpation, although it is also indicated for posttraumatic defects of the mandible. Less common indications include osteoradionecrosis and infection.
The fibula flap remains the standard for microvascular mandible reconstruction.
Although many descriptions of surgical technique exist, the closing wedge osteotomy remains a “black box” for learners.
In this chapter, a simple and reliable technique to create anatomic wedge osteotomies is presented, using preoperative templates based on the patient’s native anatomy.
ANATOMY
The anatomy relevant to fibula flap harvest is presented in Chapter 10 of this section, as well as techniques for neomandible creation using CAD/CAM osteotomy jigs.
This chapter focuses exclusively on how to create a neomandible using traditional templates and closing wedge osteotomies.
PATIENT HISTORY AND PHYSICAL FINDINGS
Risk factors for wound healing complications should be assessed, including radiation exposure, smoking, diabetes, steroid use, poor nutrition, and obesity.
Prior neck dissection can make reoperation and recipient vessel exposure difficult. A history of lower extremity trauma, surgery, or peripheral vascular disease may preclude use of the fibula flap.
The oral cavity is examined and the expected defect analyzed for quantity of bone and lining required.
Patients with poor dentition who will require adjuvant radiotherapy may benefit from dental extraction.
Occlusion is assessed and carefully noted, as one goal of surgery is to maintain native occlusion.
Distal lower extremity pulses and skin texture are examined.
Patients with potential vascular disease should undergo preoperative imaging to evaluate three-vessel runoff.
Patients with taut or thin skin will likely require a splitthickness skin graft for donor-site closure.
IMAGING
Craniofacial CT scans are performed to assess the extent of disease (tumor, traumatic defect, osteoradionecrosis, infection).
Three-dimensional renderings are helpful but not necessary.
Lower extremity angiography is commonly performed (CTA or MRA) to assess three-vessel runoff. If these studies are inadequate, conventional angiography is performed.
Patients must have at least a patent anterior tibial or posterior tibial artery (in addition to the blood supply of the flap derived from the peroneal artery) to be candidates for fibula flap harvest.
SURGICAL MANAGEMENT
Preoperative Planning
Excellent communication between the extirpative and reconstructive surgeons is necessary to coordinate perioperative planning, including staging of disease, imaging, labs, and clearance for surgery.
In delayed reconstruction, eg, in patients treated for traumatic defects, it is helpful to have two surgeons involved (one to recreate the defect and expose recipient vessels and the other to elevate the flap). However, this is not an absolute requirement.
A secure airway is required in the perioperative period, as flap swelling, abnormal deglutition, and secretions can compromise the airway. In addition, emergent reintubation may compromise microsurgical reconstruction and disrupt the repair. As a result, a tracheostomy is almost always indicated until adequate healing has occurred to allow decannulation.
Adequate nutrition is important in the perioperative period.
A flexible nasogastric or nasoduodenal tube is often placed at the end of surgery for early initiation of tube feedings.
If patients are malnourished prior to surgery, a percutaneous endoscopic gastrostomy tube may be considered.
Positioning
Patients are placed in supine position with a bump under the shoulders and the neck extended.
A folded towel or blanket is placed under the hip to facilitate internal rotation when the hip and knee are flexed.
A padded roll or IV bag is secured to the table so the foot can rest on it with the hip and knee flexed (and internally rotated). This facilitates exposure and dissection.
The heels and lower extremity are padded to avoid pressure sores during these long procedures.
The entire lower extremity is prepped and a sterile tourniquet is used so the thigh can later be used as a donor site for a split-thickness skin graft if needed.
Approach
If the defect is truly central, and both necks are available for recipient vessels, then either extremity can be utilized to harvest a fibula flap.
The left is preferable as most patients use their right leg for driving, etc., but angiographic findings may also dictate which side to use.
An ipsilateral flap (with respect to the location of the defect in the jaw) is typically used. This approach places the septum carrying the cutaneous vessel/s externally and inferiorly.
This allows the septum and skin to be brought over the hardware and into the oral cavity for standard gingiva/floor of mouth defects.
In addition, using the ipsilateral flap places the pedicle vessels laterally on the fibula flap thus localizing the vessels in optimal position for microsurgical anastomosis to the neck vessels.
A contralateral flap will place the septum and skin island internally and superiorly, which may be preferable when there is a large intraoral defect that extends beyond the gingiva/floor of mouth.
A two-team approach is preferable to reduce operative time.
The flap can be elevated during extirpation, provided there is good communication between the two operative teams and an accurate estimate of the defect is made.
It is prudent to take more flap than you think you might need.
The neomandible can be created in situ on the leg, further reducing both operative and ischemic time.
TECHNIQUES
▪ Maintaining Native Condyle Position and Occlusion
Mandibular discontinuity leads to abnormal condylar positioning and malocclusion, as the muscles of mastication contract each segment unopposed. Significant distortion of native condylar positioning when re-establishing mandibular continuity can lead to malocclusion and/or abnormal movement when chewing.
If the disease process has not distorted the outer border of the mandible, prior to resection a reconstruction bar can be appropriately bent and secured to it using two screws on the nonpathologic side of each planned extirpative osteotomy.
Following resection, the bar is replaced and the fibula flap can usually be secured to it, provided it maintains occlusion and there are not large gaps (greater than 3 mm) between the bar and fibula.
Locking screws are required when gaps exist, to prevent distortion of the bony segments and gaps between bone and bone (worse than gaps between bone and hardware).
If necessary, a new bar can be appropriately bent (using osteotomy templates) and secured, although it may be necessary to place the patient in temporary mandibulomaxillary fixation (MMF) to maintain occlusion during the revised osteosynthesis.
If the disease process has grossly distorted the external surface of the mandible, placing the patient in temporary MMF after resection will maintain condylar positioning and proper occlusion for bony inset of the fibula flap.
For edentulous patients, a reconstruction bar can be bent around the tumor and secured to the normal segments of the bone as above. This bar can be replaced with a new bar that is bent using the osteotomy templates. In this case, the initial bar should be secured to the normal segments using holes that are not near the cortex designated for final osteosynthesis.
The author’s preference is to avoid postoperative MMF if the teeth easily come into good occlusion following final flap inset.
It is unlikely that significant malocclusion following osteosynthesis of the neomandible will be corrected with MMF. Adjusting how the bony segments are secured to the hardware may be necessary to optimize native occlusion.
For edentulous patients, occlusion is not a factor and anatomic inset is not as critical.
▪ Creating Anatomic Templates
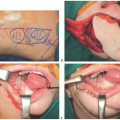
The lowest axial cut of the mandible on preoperative CT is printed and the outer surface traced and cut to create linear segments separated by distinct angles (TECH FIG 1A,B).
Mandibular angle templates are based on the appropriate sagittal image.
Although it is possible to print 1:1 (“life size”) images of the CT, the osteotomy angles are the same regardless of magnification.
A template is created for each osteotomy by tracing the printed CT onto a plastic sheet (eg, a sterile plastic bowl) that is sterilized with Betadine or chlorhexidine (TECH FIG 1C,D).
It is critical to draw the inner (lingual) lines parallel to the outer (buccal) lines and the exact same distance from them (ideally 1 cm).
The junction of these lines forms a point that is critical in subsequent steps (TECH FIG 1E).Related posts:
 Lateral Mandible Reconstruction With Soft Tissue Flaps
Lateral Mandible Reconstruction With Soft Tissue Flaps
 Repair of Lip Defects With Karapandzic Flaps
Repair of Lip Defects With Karapandzic Flaps
 Lower Eyelid Reconstruction With Palatal Grafts
Lower Eyelid Reconstruction With Palatal Grafts
 Reconstruction of the Ear Lobe
Reconstruction of the Ear Lobe
 Pectoralis Major Flap for Pharyngeal Reconstruction
Pectoralis Major Flap for Pharyngeal Reconstruction
 Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers
Facial Reanimation in the Oncologic Patient Using Nerve Grafts and Nerve Transfers

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


