Oneida Arosarena, Yadro Ducic, and Travis T. Tollefson address questions for discussion and debate:
- 1.
Is rigid fixation essential for the treatment of angle fractures, or is a single plate along the superior border sufficient?
- 2.
Does the presence of teeth in the fracture line (particularly the third molar in angle fractures) contribute to stability of the fixation, or is it a nidus for infection?
- 3.
What is the role of postoperative antibiotics? Are they always necessary?
- 4.
Do you believe that applying MMF is an important part of mandibular fracture repair? If you do not use MMF in all cases, how do you decide which cases require intraoperative and/or postoperative MMF? Do you believe that the techniques/methods of applying MMF make a difference?
- 5.
How do you manage edentulous mandible fractures?
- 6.
Analysis: Over the past 5 years, how has your technique or approach changed or what is the most important thing you have learned in dealing with mandible fractures?
Oneida Arosarena, Yadro Ducic, and Travis T. Tollefson address questions for discussion and debate:
- 1.
- 2.
- 3.
What is the role of postoperative antibiotics? Are they always necessary?
- 4.
- 5.
How do you manage edentulous mandible fractures ?
- 6.
Is rigid fixation essential for the treatment of angle fractures, or is a single plate along the superior border sufficient?
Arosarena
Because of the biomechanics of the mandible, mandibular angle fractures have a high incidence of postsurgical complications. There are currently 2 philosophies espoused by practitioners who use open reduction and internal fixation (ORIF) in the treatment of mandibular angle fractures.
Philosophy 1. The goal of the first group is rigid fixation with 2 miniplates resulting in primary bone union, which necessitates absolute immobility of the fracture fragments according to older Arbeitsgemeinschaft für Osteosynthesefragen–Association for the Study of Internal Fixation guidelines.
Philosophy 2. The second group advocates the use of a single miniplate along the ideal line of osteosynthesis as described by Champy. Although this method does not result in rigid fixation, its proponents list benefits of decreased soft-tissue stripping that maintains blood supply to the mandible, the lack of an external incision, and cost savings related to decreased operative time and savings in hardware. Because bite forces do not return to premorbid levels for several weeks after fracture treatment, proponents of the Champy technique argue that absolute rigid fixation may not be necessary for angle fractures.
Several biomechanical studies have demonstrated that the Champy technique has less favorable biomechanical behavior than biplanar plating techniques. Two studies revealed that a 3-dimensional plate at the superior border of the mandible resulted in increased stability with torsional loading when compared with other commonly used mandibular angle fixation techniques, effecting biplanar fixation with a single plate. However, these studies may represent oversimplified depictions of fractured mandible biomechanics, not taking into account the stabilizing effects of surrounding tissues, particularly muscles. Moreover, these models do not take into account the possibility of stress shielding in the healing mandible that could be attributed to rigid fixation.
In a prospective, randomized trial of 54 patients with unilateral, isolated mandibular angle fractures, Danda found that the use of 2 noncompression miniplates had no advantage over the use of 1 superior border plate, and that the use of 2 miniplates resulted in scarring at the transcutaneous incision in 18% of patients. However, Danda used 2 weeks of interdental fixation in all patients. Similarly, in a study of 185 patients with isolated unilateral angle fractures, Ellis found no significant difference in treatment outcomes for patients treated with rigid versus nonrigid fixation, although patients treated with rigid fixation in this study had longer operative times and more wound problems. A recent meta-analysis of mandibular angle fixation techniques found lower complication rates with the use of 1 superior border plate compared with the use of 2 plates.
Ducic
The decision as to which method of fixation is most appropriate will, of course, be determined by the specific type of injury present. There are several options in treating these injuries with respect to fixation modality. Closed reduction is still an option. However, there is a prolonged period of immobilization that may be associated with increased rate of long-term temporomandibular joint problems. Closed reduction is relatively contraindicated in comminuted angle fractures because of the increased risk of complications. Rigid load-bearing plating of angle fractures is needed in comminuted fractures. Compression plating and lag screw fixation is not appropriate in these circumstances, because of the potential for fragmentary telescoping. Studies performed in noncomminuted angle fractures demonstrate a decreased risk of complications with a single superior border monocortical miniplate placed along Champy’s ideal line of osteosynthesis, slightly greater complication rate with an inferior border bicortical plate, and the greatest rate of complications with 2 separate plates.
Tollefson
In treatment of fractures of craniomaxillofacial skeleton, is it not rigid truth that 2 plates are better than 1? Unfortunately, the relationship of bioengineering concepts to the clinical application of rigid fixation is not as linear as we would expect. Practice patterns in mandible fracture management have steadily evolved over the last century, with surges of major advances from both bioengineering and clinical fields. Ellis recently reported superiority of the single miniplate technique for mandibular angle fractures over either maxillomandibular fixation after closed reduction or 2-plate fixation. He cited fewer complications and shorter operative time. I concur with the application of a single plate at the mandibular oblique line for treatment of angle fractures in the following circumstances:
- 1.
Adequate bone stock is available
- 2.
Comminution or bone defect (eg, gunshot wound) is not present
- 3.
Nonedentulous
- 4.
In the presence of adequate dentition to restore occlusion.
I will briefly introduce the state of the science by reviewing the theories of rigid versus adaptive fixation and the reports of the outcomes of their application.
Without considering the extremes of treatment trends, the contemporary history of mandible fracture treatment paradigms can be simplified into 2 different schools:
- 1.
Treatment patterns restricting function and movement (with external fixation, wires, and load-bearing internal fixation)
- 2.
Shift to near immediate return to function with limited, site-directed internal plate fixation.
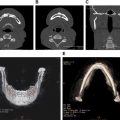
The latter incorporates the concept of adaptive osteosynthesis, which has come to be colloquially referred to as the Champy technique in reference to his expansion on the work of Michelet ( Fig. 1 ). The former, adapted from Association for Osteosynthesis/Association for the Study of Internal Fixation (AO-ASIF) orthopedic management principles of long bone fractures, is supported because of the establishment of rigid fixation for primary bone healing by limiting motion around the fracture ( Figs. 1–4 ).


Conflicting clinical outcomes have been reported using principles of either school, but the fracture site, complexity of the forces applied to the fracture, and independent patient characteristics must be considered. Ellis and Walker reported on angle fracture fixation with 2 miniplates, but later suggested a lower complication rate with a single miniplate. The investigators partially attributed this difference to the additional dissection needed for the second plate. Fox and Kellman contrasted this report with a 2.9% complication rate in 70 angle fractures treated with 2 monocortical miniplates, and also clarified that the 1994 Ellis and Walker study included bicortical application of the inferior border plate. As with any comparative effectiveness research, a direct, randomized prospective study of sufficient power would be ideal, but is unlikely. It is plausible that these contrasting clinical experiences may be clarified by studying outcomes in a multi-institutional database with sufficient collection of fracture details and related secondary factors of bone healing, such as soft-tissue dissection, approaches, technique, and duration of maxillomandibular fixation, and the general patient’s general “protoplasm” or health (eg, diabetes, alcoholism, malnutrition, tobacco abuse).
Although the contrasting clinical reports can be difficult to directly compare, I am comfortable with the relative success using either 1 or 2 miniplates on the mandibular angle. I strongly concur with Rudderman and colleagues in that fixation should “provide for a functional construct that can adequately heal while the patient participates in near normal activities.” It may seem contradictory to suggest that less fixation is better in some circumstances, but applying functionally stable fixation while allowing dental loads to be applied to the healing mandible may improve bone density, as described by Julius Wolff in 1892 in the law of transformation of bone. The 1-plate technique on the oblique line is my preference for the uncomplicated mandibular angle fracture because it adequately minimizes interfragmentary movement via a limited soft-tissue dissection.
Does the presence of teeth in the fracture line (particularly the third molar in angle fractures) contribute to stability of the fixation, or is it a nidus for infection?
Arosarena
The prophylactic removal of teeth in the line of fracture was advocated before the widespread use of antibiotics and rigid internal fixation, both of which have significantly reduced the infection rate associated with repair of mandible fractures. Retained teeth historically were believed to act as foreign bodies, providing communication between the oral cavity and the periodontal space. The trend over time has been retention of viable teeth in the fracture line.
Ellis reported a trend toward increased complication rates when molars, particularly the third molar, are involved in the fracture line. However, at least 3 retrospective series demonstrated no difference in outcome of fracture management whether the teeth were routinely extracted or retained, and regardless of whether the fracture was in the anterior or posterior dentition. The third molar may represent a different situation because it is in a region where debris tends to collect. In a retrospective analysis of 105 mandible fractures associated with incompletely erupted third molars, Rubin and colleagues found a trend toward increased complication rates in cases treated with open reduction when the third molar was retained. Other investigators recommend retention of healthy third molars that do not interfere with fracture reduction, particularly unerupted third molars. They argue that extraction of the third molar reduces contact area in the already thin angular region of the mandible, which may reduce the stability of osteosynthesis and cause micromobility after fixation.
Extraction of viable teeth may induce additional trauma to the adjacent bone and destabilize the fracture. In addition, healthy retained teeth provide a posterior stop, permit proper alignment of the dental arch, and prevent collapsing or telescoping of the fragments. Moreover, a normal coagulum does not always form after tooth extraction, occasionally leading to alveolitis and wound infection. According to Spinnato and Alberto, conditions for preserving teeth in the fracture line are antibiotic therapy, strict oral hygiene, radiologic and clinical monitoring for evidence of periapical infection and pulp necrosis, and endodontic therapy for teeth that require treatment. Widely accepted indications for removal of the teeth in the line of fracture include :
- •
Significant periodontal disease with gross mobility and periapical pathology
- •
Partially erupted or erupted third molars with pericoronitis or cystic areas
- •
Teeth preventing the reduction of fractures
- •
Teeth with fractured roots
- •
Teeth with exposed root apices or teeth in which the entire root surface from the apex to the gingival margin is exposed
- •
Excessive delay from the time of fracture to the time of definitive treatment
- •
Recurring abscess at the fracture site despite antibiotic therapy.
Ducic
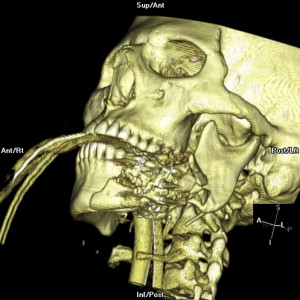
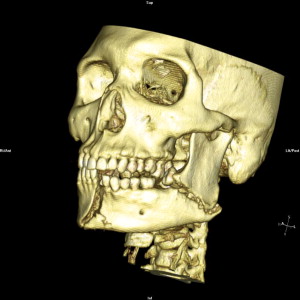
The presence of a third molar doubles the risk of mandible fracture because of the sheer volume of bone it occupies, effectively diminishing the height of the remaining mandible. There does exist some controversy as to the need for third molar extraction in the setting of mandibular angle fractures. Indications for removal are generally accepted to include the presence of a fractured tooth, a carious tooth, grossly loose or displaced tooth, an impacted third molar that would meet criteria for removal on its own merit, and a tooth preventing adequate fracture reduction. This latter scenario is most often seen with a preoperatively impacted third molar ( Figs. 2 and 3 ). If none of these criteria are met then one may consider retaining the tooth based on intraoperative factors. Removing third molars may further diminish the amount of bone remaining across the fracture site and may make the stability of the reduction less stable; this is an intraoperative decision. Several studies support this approach.
Tollefson
Controversy persists over whether to remove a third molar that is in a mandibular angle fracture line. Before the advent of antibiotics, infections in fractures along the tooth-bearing mandible were common. Tooth extraction from the fracture site theoretically decreased bacterial load, but the advent of antibiotics shifted the paradigm. My practice is to retain healthy, erupted molars in mandibular angle fractures with the exception of the indications that I will further describe.
As infection-related complications decreased with the routine use of preoperative and perioperative antibiotics, surgeons began to sort through the effectiveness of different practice patterns: tooth extraction, duration of maxillomandibular fixation, rigid versus adaptive osteosynthesis, and surgical approaches. The debate over third molar extraction in angle fractures excludes an abscessed or severely decayed tooth, which should be extracted in fractures of any area of the mandible. This clinical debate is also partially fueled by the routine practice of preventive extraction of third molar or wisdom teeth, which have had evolving indications and justifications in the oral surgery literature.
Third molars, occupying significant cross-sectional area of the mandibular angle, have been shown to predispose patients to up to 3.8 times the risk of angle fractures than those without third molars. Once the fracture is present, some surgeons choose to extract, whereas others retain the third molar. I concur with the theory that extraction of the third molar from a fracture line may destabilize and limit the interfragmentary buttressing required for bone healing ( Fig. 4 ).
The literature has support for both extraction and retention of the third molars in angle fractures. The support in the literature for retention is strong. Neal and colleagues and Amaratunga found that removing teeth in the line of a fracture did not change infection rates. The investigators included other tooth-bearing fracture locations in the studies, so we must infer how the angle fractures would behave. Iizuka and Lindqvist went further to suggest that tooth extraction can contribute to postoperative infection. These investigators purport that the tooth extraction may make the fracture site unstable because of diminished bone stock, whereas retaining a tooth may add to stability. In a later study of 121 angle fractures, infection risk was higher after tooth extraction in the fracture line and when compression plate technique was used. The latter practice is now rare.
The support for routine third molar extraction from the fracture line is less convincing. In 1964, Muller supported extraction of teeth with multiple roots from fracture lines. Ellis recently reviewed 400 cases in which third molar extraction from the angle fracture was routine practice. Third molars in the fracture line were present in 85% of the fractures, and 75% of these teeth were removed. Although the difference in infection and complication rates failed to reach statistical significance, he concludes that the “difficulty that remains involves determining the appropriate criteria for the removal of teeth in the line of fracture.” (p865)
Determining the criteria for extraction remains challenging. My current practice is to retain the third molar in the mandibular fracture line except when the roots are fractured, ( Fig. 5 ) severe dental caries and mobility are present, or in the presence of pericoronitis, abscess, or infection. If extraction of the third molar is required, it can be removed after bone healing, as suggested by Iizuka and Lindquist.

Does the presence of teeth in the fracture line (particularly the third molar in angle fractures) contribute to stability of the fixation, or is it a nidus for infection?
Arosarena
The prophylactic removal of teeth in the line of fracture was advocated before the widespread use of antibiotics and rigid internal fixation, both of which have significantly reduced the infection rate associated with repair of mandible fractures. Retained teeth historically were believed to act as foreign bodies, providing communication between the oral cavity and the periodontal space. The trend over time has been retention of viable teeth in the fracture line.
Ellis reported a trend toward increased complication rates when molars, particularly the third molar, are involved in the fracture line. However, at least 3 retrospective series demonstrated no difference in outcome of fracture management whether the teeth were routinely extracted or retained, and regardless of whether the fracture was in the anterior or posterior dentition. The third molar may represent a different situation because it is in a region where debris tends to collect. In a retrospective analysis of 105 mandible fractures associated with incompletely erupted third molars, Rubin and colleagues found a trend toward increased complication rates in cases treated with open reduction when the third molar was retained. Other investigators recommend retention of healthy third molars that do not interfere with fracture reduction, particularly unerupted third molars. They argue that extraction of the third molar reduces contact area in the already thin angular region of the mandible, which may reduce the stability of osteosynthesis and cause micromobility after fixation.
Extraction of viable teeth may induce additional trauma to the adjacent bone and destabilize the fracture. In addition, healthy retained teeth provide a posterior stop, permit proper alignment of the dental arch, and prevent collapsing or telescoping of the fragments. Moreover, a normal coagulum does not always form after tooth extraction, occasionally leading to alveolitis and wound infection. According to Spinnato and Alberto, conditions for preserving teeth in the fracture line are antibiotic therapy, strict oral hygiene, radiologic and clinical monitoring for evidence of periapical infection and pulp necrosis, and endodontic therapy for teeth that require treatment. Widely accepted indications for removal of the teeth in the line of fracture include :
- •
Significant periodontal disease with gross mobility and periapical pathology
- •
Partially erupted or erupted third molars with pericoronitis or cystic areas
- •
Teeth preventing the reduction of fractures
- •
Teeth with fractured roots
- •
Teeth with exposed root apices or teeth in which the entire root surface from the apex to the gingival margin is exposed
- •
Excessive delay from the time of fracture to the time of definitive treatment
- •
Recurring abscess at the fracture site despite antibiotic therapy.
Ducic
The presence of a third molar doubles the risk of mandible fracture because of the sheer volume of bone it occupies, effectively diminishing the height of the remaining mandible. There does exist some controversy as to the need for third molar extraction in the setting of mandibular angle fractures. Indications for removal are generally accepted to include the presence of a fractured tooth, a carious tooth, grossly loose or displaced tooth, an impacted third molar that would meet criteria for removal on its own merit, and a tooth preventing adequate fracture reduction. This latter scenario is most often seen with a preoperatively impacted third molar ( Figs. 2 and 3 ). If none of these criteria are met then one may consider retaining the tooth based on intraoperative factors. Removing third molars may further diminish the amount of bone remaining across the fracture site and may make the stability of the reduction less stable; this is an intraoperative decision. Several studies support this approach.
Tollefson
Controversy persists over whether to remove a third molar that is in a mandibular angle fracture line. Before the advent of antibiotics, infections in fractures along the tooth-bearing mandible were common. Tooth extraction from the fracture site theoretically decreased bacterial load, but the advent of antibiotics shifted the paradigm. My practice is to retain healthy, erupted molars in mandibular angle fractures with the exception of the indications that I will further describe.
As infection-related complications decreased with the routine use of preoperative and perioperative antibiotics, surgeons began to sort through the effectiveness of different practice patterns: tooth extraction, duration of maxillomandibular fixation, rigid versus adaptive osteosynthesis, and surgical approaches. The debate over third molar extraction in angle fractures excludes an abscessed or severely decayed tooth, which should be extracted in fractures of any area of the mandible. This clinical debate is also partially fueled by the routine practice of preventive extraction of third molar or wisdom teeth, which have had evolving indications and justifications in the oral surgery literature.
Third molars, occupying significant cross-sectional area of the mandibular angle, have been shown to predispose patients to up to 3.8 times the risk of angle fractures than those without third molars. Once the fracture is present, some surgeons choose to extract, whereas others retain the third molar. I concur with the theory that extraction of the third molar from a fracture line may destabilize and limit the interfragmentary buttressing required for bone healing ( Fig. 4 ).
The literature has support for both extraction and retention of the third molars in angle fractures. The support in the literature for retention is strong. Neal and colleagues and Amaratunga found that removing teeth in the line of a fracture did not change infection rates. The investigators included other tooth-bearing fracture locations in the studies, so we must infer how the angle fractures would behave. Iizuka and Lindqvist went further to suggest that tooth extraction can contribute to postoperative infection. These investigators purport that the tooth extraction may make the fracture site unstable because of diminished bone stock, whereas retaining a tooth may add to stability. In a later study of 121 angle fractures, infection risk was higher after tooth extraction in the fracture line and when compression plate technique was used. The latter practice is now rare.
The support for routine third molar extraction from the fracture line is less convincing. In 1964, Muller supported extraction of teeth with multiple roots from fracture lines. Ellis recently reviewed 400 cases in which third molar extraction from the angle fracture was routine practice. Third molars in the fracture line were present in 85% of the fractures, and 75% of these teeth were removed. Although the difference in infection and complication rates failed to reach statistical significance, he concludes that the “difficulty that remains involves determining the appropriate criteria for the removal of teeth in the line of fracture.” (p865)
Determining the criteria for extraction remains challenging. My current practice is to retain the third molar in the mandibular fracture line except when the roots are fractured, ( Fig. 5 ) severe dental caries and mobility are present, or in the presence of pericoronitis, abscess, or infection. If extraction of the third molar is required, it can be removed after bone healing, as suggested by Iizuka and Lindquist.